Physiologic Evaluation of Microvascular Damage in Culprit Vessel After Successful Primary Percutaneous Coronary Intervention for ST-elevation Myocardial Infarction Patients
- Affiliations
-
- 1Heart Vascular Stroke Institute, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. drone80@hanmail.net
- KMID: 2385844
- DOI: http://doi.org/10.12997/jla.2017.6.1.46
Abstract
- We investigated the importance of comprehensive physiologic assessment about culprit vessel in STEMI in estimating long-term clinical outcomes after complete revascularization. Comprehensive physiologic assessment provides additional information about microvascular function in coronary artery disease. This assessment includes three indices, fractional flow reserve (FFR), index of microcirculatory resistance (IMR) and coronary flow reserve (CFR). We have performed the comprehensive physiologic assessment in culprit vessels after successful primary PCI in STEMI patients. Both cases were thrombotic total occlusion in mid right coronary artery with inferior wall STEMI, successfully revascularized with stent implantation after thrombus suction. However, in post PCI physiologic assessment, one case showed overt microvascular damage. CFR was 1.1, and IMR was 75U, which was defined as a combined criterion of low CFR (<2.0) and high IMR (≥25U) in culprit vessel, but the other case showed 2.2 in CFR and 24U in IMR, which suggested no overt microvascular damage. Moreover, we can validate these findings by cardiac MR after primary PCI. Previous studies presented that the presence of overt microvascular damage was significantly associated with worse clinical outcome in patients with coronary artery disease. We suggest that comprehensive physiologic evaluation provides important information about the degree of microvascular damage and long-term clinical outcomes after complete revascularization in culprit vessel in STEMI.
Keyword
MeSH Terms
Figure
-

Fig. 1 Initial EKG in Case 1. There is ST elevation in lead II, III, aVF with reciprocal change in V4-6.
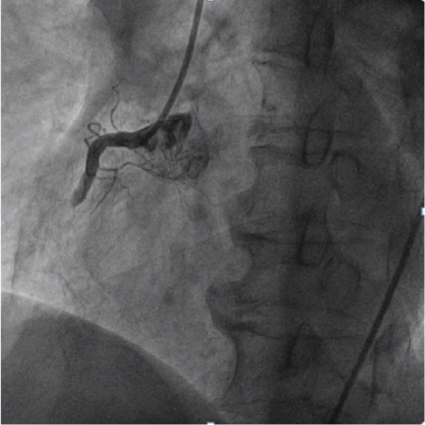
Fig. 2 Coronary angiography of culprit vessel in Case 1. Total thrombotic occlusion was seen in mid right coronary artery (RCA).
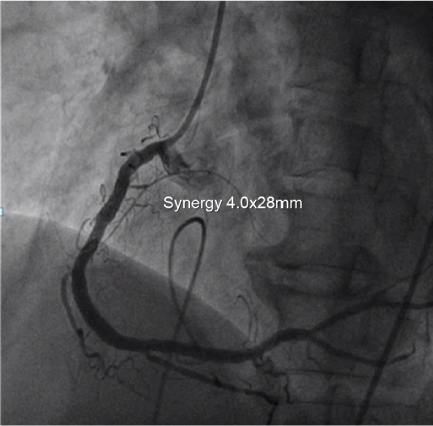
Fig. 3 Coronary angiography after successful revascularization in Case 1. We performed PCI with stent implantation, Synergy 4.0×28 mm.
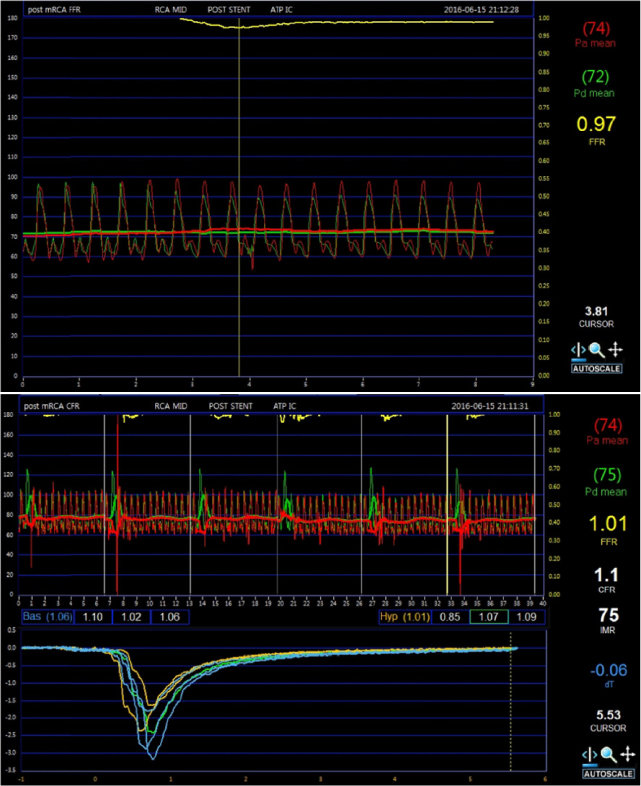
Fig. 4 Post-PCI Physiologic assessment in culprit vessel in Case 1. CFR was depressed to 1.1 and IMR was elevated up to 75 U.
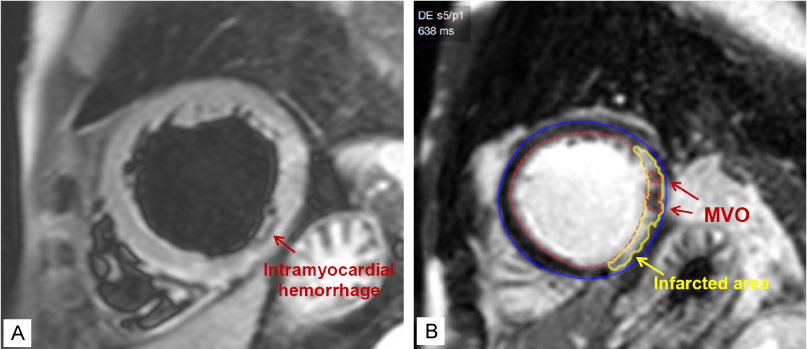
Fig. 5 Cardiac MR 5 days after primary PCI in Case 1. (A) Intramyocardial hemorrhage was seen in T2 weighted image, (B) Microvascular obstruction in Late gadolinium enhancement.

Fig. 6 Initial EKG in Case 2. There is ST elevation in II, III, aVF with reciprocal changes with V2-4.

Fig. 7 Coronary angiography in Case 2. Thrombotic total occlusion was seen in mid right coronary artery (RCA).
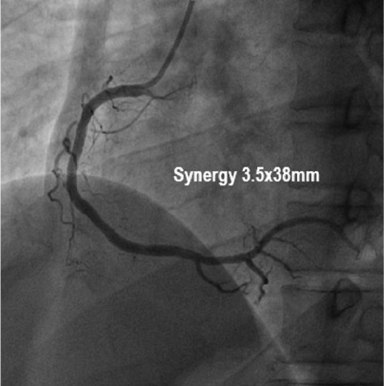
Fig. 8 Coronary angiography after Successful Revascularization in Case 2. We performed PCI with stent implantation, Synergy 3.5×38 mm.
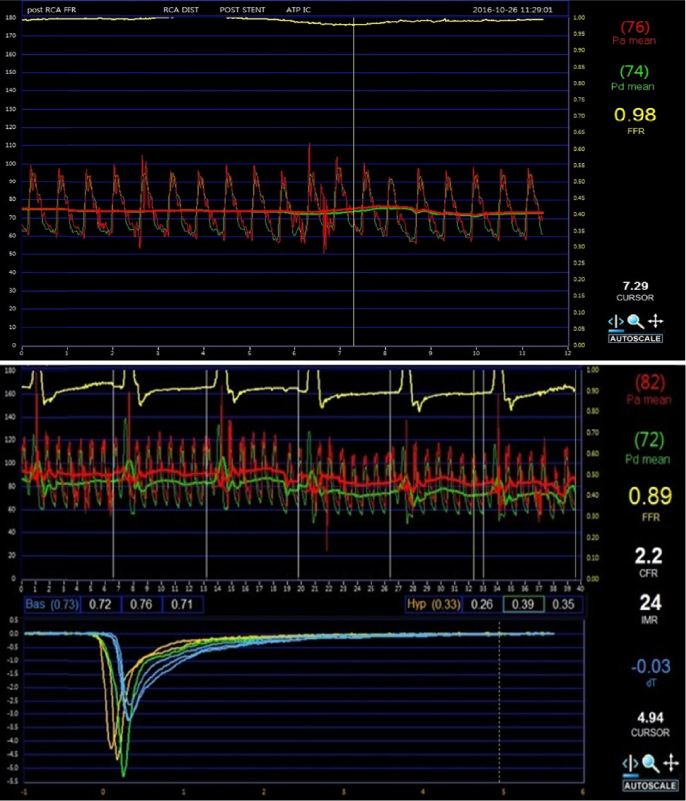
Fig. 9 Post-PCI Comprehensive Physiologic Assessment in Culprit Vessel in Case 2. CFR was 2.2 and IMR was 24 U.
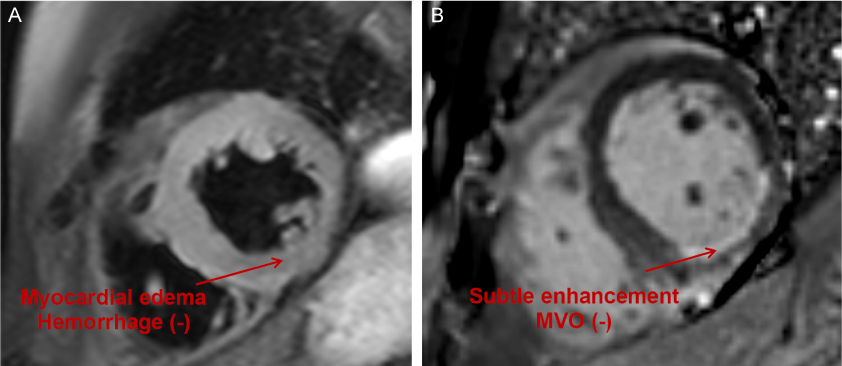
Fig. 10 Cardiac MR in 2 days after post-PCI in Case 2. (A) No myocardial hemorrhage in T2 weighted image, (B) Only subtle enhancement was seen in Late gadolinium enhancement
Reference
-
1. Fearon WF, Low AF, Yong AS, McGeoch R, Berry C, Shah MG, et al. Prognostic value of the index of microcirculatory resistance measured after primary percutaneous coronary intervention. Circulation. 2013; 127:2436–2441.
Article2. McGeoch R, Watkins S, Berry C, Steedman T, Davie A, Byrne J, et al. The index of microcirculatory resistance measured acutely predicts the extent and severity of myocardial infarction in patients with ST-segment elevation myocardial infarction. JACC Cardiovasc Interv. 2010; 3:715–722.
Article3. van de Hoef TP, Bax M, Meuwissen M, Damman P, Delewi R, de Winter RJ, et al. Impact of coronary microvascular function on long-term cardiac mortality in patients with acute ST-segment-elevation myocardial infarction. Circ Cardiovasc Interv. 2013; 6:207–215.
Article4. Lee JM, Jung JH, Hwang D, Park J, Fan Y, Na SH, et al. Coronary flow reserve and microcirculatory resistance in patients with intermediate coronary stenosis. J Am Coll Cardiol. 2016; 67:1158–1169.
Article5. Lim HS, Yoon MH, Tahk SJ, Yang HM, Choi BJ, Choi SY, et al. Usefulness of the index of microcirculatory resistance for invasively assessing myocardial viability immediately after primary angioplasty for anterior myocardial infarction. Eur Heart J. 2009; 30:2854–2860.
Article6. Park SD, Baek YS, Lee MJ, Kwon SW, Shin SH, Woo SI, et al. Comprehensive assessment of microcirculation after primary percutaneous intervention in ST-segment elevation myocardial infarction: insight from thermodilution-derived index of microcirculatory resistance and coronary flow reserve. Coron Artery Dis. 2016; 27:34–39.
Article7. Fearon WF, Balsam LB, Farouque HM, Caffarelli AD, Robbins RC, Fitzgerald PJ, et al. Novel index for invasively assessing the coronary microcirculation. Circulation. 2003; 107:3129–3132.
Article8. Ng MK, Yeung AC, Fearon WF. Invasive assessment of the coronary microcirculation: superior reproducibility and less hemodynamic dependence of index of microcirculatory resistance compared with coronary flow reserve. Circulation. 2006; 113:2054–2061.
Article9. Fearon WF, Shah M, Ng M, Brinton T, Wilson A, Tremmel JA, et al. Predictive value of the index of microcirculatory resistance in patients with ST-segment elevation myocardial infarction. J Am Coll Cardiol. 2008; 51:560–565.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Consecutive Multivessel Myocardial Infarction during Primary Percutaneous Coronary Intervention
- Missing Right Coronary Artery in a Patient with Acute Inferior ST Segment Elevation Myocardial Infarction: A Case of Extremely Rare Variation of Coronary Anatomy
- Current Status of Coronary Intervention in Patients with ST-Segment Elevation Myocardial Infarction and Multivessel Coronary Artery Disease
- Two Cases of Complications during Percutaneous Coronary Intervention for Myocardial Infarction in Patients with Concurrent Chronic Total Occlusion in an Emergency Setting
- Successful Primary Percutaneous Coronary Intervention without Stenting: Insight from Optimal Coherence Tomography
