Additive Role of Coronary Magnetic Resonance Angiography for the Evaluation of Coronary Artery Disease
- Affiliations
-
- 1Department of Cardiology, Cardiovascular Center, Seoul National University Bundang Hospital, Seongnam, Korea. yeonyeeyoon@snubh.org
- 2Department of Radiology, Cardiovascular Center, Seoul National University Bundang Hospital, Seongnam, Korea.
- KMID: 2385396
- DOI: http://doi.org/10.4070/kcj.2016.0288
Abstract
- Coronary magnetic resonance angiography (CMRA) allows a noninvasive assessment of the coronary anatomy without exposing the patients to radiation. It is also superior to coronary computed tomography angiography (CCTA) for the evaluation of luminal narrowing in heavily calcified coronary segments. We report a case with triple-vessel disease, but it could not be accurately assessed by CCTA because of calcification and lack of a significant perfusion defect or myocardial scarring on cardiac magnetic resonance imaging (MRI). However, whole-heart CMRA performed as part of the cardiac MRI protocol demonstrated significant triple-vessel disease with left main involvement, confirmed by subsequent invasive angiography with a fractional flow reserve measurement.
MeSH Terms
Figure
-
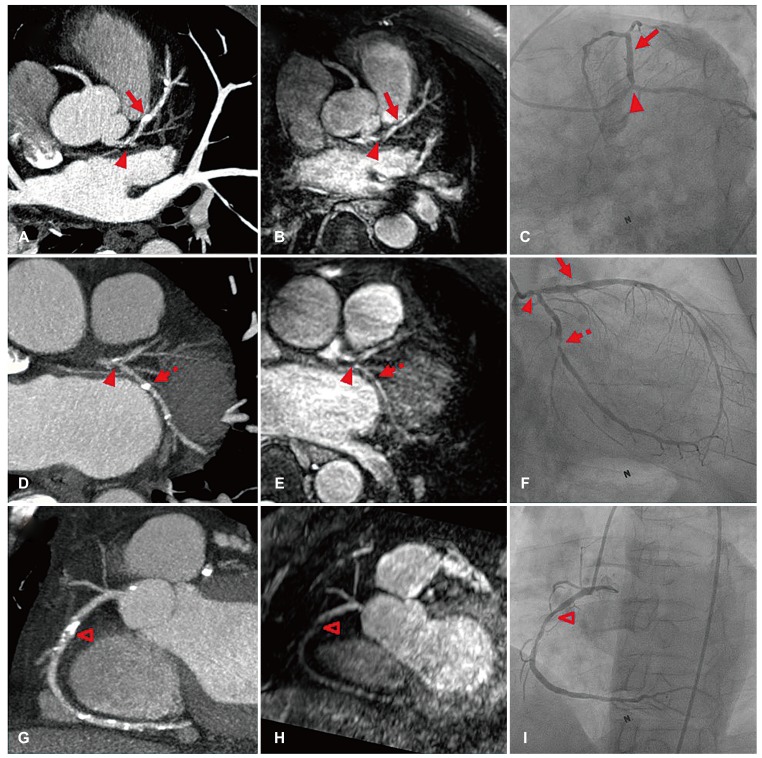
Fig. 1 CCTA, CMRA, and invasive CAG findings. CCTA revealed multifocal coronary artery disease in the left main bifurcation (A, D, arrowheads), proximal left anterior descending artery (A, arrow), proximal left circumflex artery (D, dotted arrow), and mid right coronary artery (G, open arrowhead). Although the CCTA evaluation of the stenosis severity was limited because of calcification (A, D, G), whole-heart CMRA demonstrated significant stenoses of the left main bifurcation (B, E, arrowheads), proximal left circumflex artery (E, dotted arrow), and mid right coronary artery (H, open arrowhead). On the other hand, the calcified plaque in the proximal left anterior descending artery was indicated as an insignificant lesion on CMRA (B, arrow). Good agreement was observed between CMRA and subsequent CAG (C, F, I). CCTA: coronary computed tomography angiography, CMRA: coronary magnetic resonance angiography, CAG: coronary angiography.
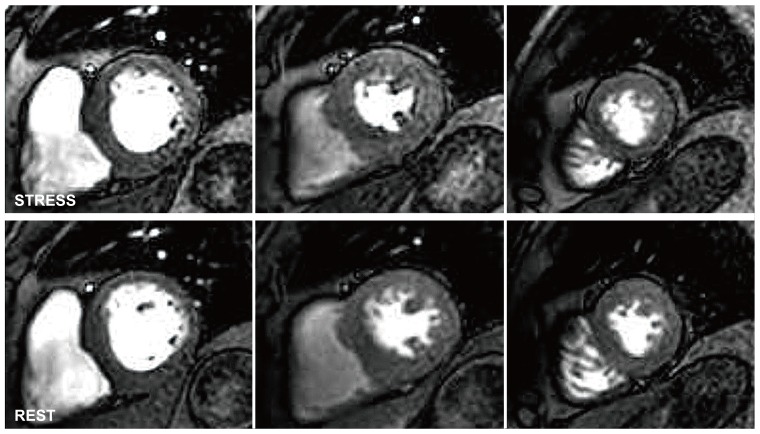
Fig. 2 Stress and rest myocardial perfusion magnetic resonance imaging findings. There was no evidence of inducible myocardial ischemia on myocardial perfusion magnetic resonance imaging (Also see Supplementary Video. 1, 2, 3, 4, 5, 6 in the online-only Data Supplement).
Reference
-
1. Sakuma H. Coronary CT versus MR angiography: the role of MR angiography. Radiology. 2011; 258:340–349. PMID: 21273518.2. Yoon YE, Hong YJ, Kim HK, et al. 2014 Korean guidelines for appropriate utilization of cardiovascular magnetic resonance imaging: a joint report of the Korean society of cardiology and the Korean society of radiology. Korean Circ J. 2014; 44:359–385. PMID: 25469139.3. Kato S, Kitagawa K, Ishida N, et al. Assessment of coronary artery disease using magnetic resonance coronary angiography: a national multicenter trial. J Am Coll Cardiol. 2010; 56:983–991. PMID: 20828652.4. Schuijf JD, Achenbach S, de Feyter PJ, Bax JJ. Current applications and limitations of coronary computed tomography angiography in stable coronary artery disease. Heart. 2011; 97:330–337. PMID: 21258119.5. Schroeder S, Achenbach S, Bengel F, et al. Cardiac computed tomography: indications, applications, limitations, and training requirements: report of a writing group deployed by the working group nuclear cardiology and cardiac CT of the European society of cardiology and the European council of nuclear cardiology. Eur Heart J. 2008; 29:531–556. PMID: 18084017.6. Chung SY, Lee KY, Chun EJ, et al. Comparison of stress perfusion MRI and SPECT for detection of myocardial ischemia in patients with angiographically proven three-vessel coronary artery disease. AJR Am J Roentgenol. 2010; 195:356–362. PMID: 20651190.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cardiac MR Assessment of Coronary Arteries
- Demonstration of Pathologic Coronary Flow Dynamics using Transthoracic Doppler Echocardiography: Its Potential Role in Clinical Decision-Making
- Spontaneous Coronary Artery Dissection and Woven Coronary Artery: Three Cases and a Review of the Literature
- Direct Visualization of Coronary Artery and Flow using Transthoracic Doppler Echocardiography
- A Case of Single Coronary Artery c Effort Angina
