The Validity of Ultrasonography-Guided Fine Needle Aspiration Biopsy in Thyroid Nodules 4 cm or Larger Depends on Ultrasonography Characteristics
- Affiliations
-
- 1Department of Endocrinology and Metabolism, Chosun University Hospital, Chosun University School of Medicine, Gwangju, Korea.
- 2Division of Endocrinology and Metabolism, Department of Medicine, Sungkyunkwan University School of Medicine, Seoul, Korea. swkimmd@skku.edu
- 3Department of Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2384253
- DOI: http://doi.org/10.3803/EnM.2014.29.4.545
Abstract
- BACKGROUND
The objective of this study was to evaluate the validity of fine needle aspiration biopsy (FNAB) according to ultrasonography (US) characteristics in thyroid nodules 4 cm and larger.
METHODS
We retrospectively reviewed the cases of 263 patients who underwent thyroid surgery for thyroid nodules larger than 4 cm between January 2001 and December 2010.
RESULTS
The sensitivity of US-FNAB was significantly higher in nodules with calcifications (micro- or macro-) than those without (97.9% vs. 87.% P<0.05). The accuracy of US-FNAB was higher in large thyroid nodules with US features suspicious of malignancy, such as a solid component, ill-defined margin, hypoechogenicity or marked hypoechogenicity, or any calcifications (micro- or macro-) compared to thyroid nodules with none of these features. Furthermore, the accuracy improved as the number of these features increased. The overall false negative rate (FNR) was 11.9%. The FNR of thyroid nodules that appeared benign on US, such as mixed nodules (7.7%) or nodules without calcification (9.8%), trended toward being lower than that of solid nodules (17.9%) or nodules with any microcalcification or macrocalcification (33.3%). In nodules without suspicious features of malignancy, the FNR of US-FNAB was 0% (0/15).
CONCLUSION
We suggest individualized strategies for large thyroid nodules according to US features. Patients with benign FNAB can be followed in the absence of any malignant features in US. However, if patients exhibit any suspicious features, potential false negative results of FNAB should be kept in mind and surgery may be considered.
MeSH Terms
Figure
-

Fig. 1 Malignancy rate according to ultrasonography-guided fine needle aspiration biopsy (FNAB) and ultrasonography characteristics, including component, margin, echogenicity, and calcification. SM, suspicious for malignancy; M, malignancy; Iso, isoechogenicity; Hypo, hypoechogenicity; MH, marked hypoechogenicity; Micro, microcalcification; Macro, macrocalcification.
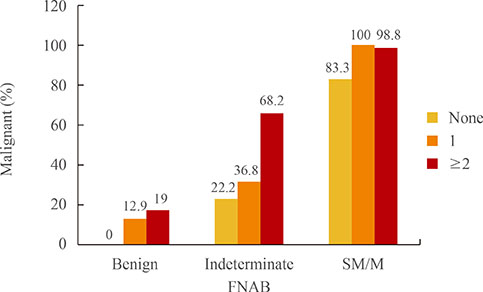
Fig. 2 Malignancy rate according to ultrasonography-guided fine needle aspiration biopsy (FNAB) and number of ultrasonography features, including solid component, ill-defined margin, hypoechogenicity or marked hypoechogenicity, and microcalcification or macrocalcification. SM, suspicious for malignancy; M, malignancy.
Cited by 1 articles
-
Risk of Malignancy in Thyroid Nodules 4 cm or Larger
Uchechukwu C. Megwalu
Endocrinol Metab. 2017;32(1):77-82. doi: 10.3803/EnM.2017.32.1.77.
Reference
-
1. Hegedus L. Clinical practice. The thyroid nodule. N Engl J Med. 2004; 351:1764–1771.2. Davies L, Welch HG. Increasing incidence of thyroid cancer in the United States, 1973-2002. JAMA. 2006; 295:2164–2167.3. American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer. Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel SJ, Mazzaferri EL, McIver B, Pacini F, Schlumberger M, Sherman SI, Steward DL, Tuttle RM. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009; 19:1167–1214.4. Nam-Goong IS, Kim HY, Gong G, Lee HK, Hong SJ, Kim WB, Shong YK. Ultrasonography-guided fine-needle aspiration of thyroid incidentaloma: correlation with pathological findings. Clin Endocrinol (Oxf). 2004; 60:21–28.5. Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel SJ, Mazzaferri EL, McIver B, Sherman SI, Tuttle RM. American Thyroid Association Guidelines Taskforce. Management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2006; 16:109–142.6. Carrillo JF, Frias-Mendivil M, Ochoa-Carrillo FJ, Ibarra M. Accuracy of fine-needle aspiration biopsy of the thyroid combined with an evaluation of clinical and radiologic factors. Otolaryngol Head Neck Surg. 2000; 122:917–921.7. McCoy KL, Jabbour N, Ogilvie JB, Ohori NP, Carty SE, Yim JH. The incidence of cancer and rate of false-negative cytology in thyroid nodules greater than or equal to 4 cm in size. Surgery. 2007; 142:837–844.8. Pinchot SN, Al-Wagih H, Schaefer S, Sippel R, Chen H. Accuracy of fine-needle aspiration biopsy for predicting neoplasm or carcinoma in thyroid nodules 4 cm or larger. Arch Surg. 2009; 144:649–655.9. Wharry LI, McCoy KL, Stang MT, Armstrong MJ, LeBeau SO, Tublin ME, Sholosh B, Silbermann A, Ohori NP, Nikiforov YE, Hodak SP, Carty SE, Yip L. Thyroid nodules (≥4 cm): can ultrasound and cytology reliably exclude cancer? World J Surg. 2014; 38:614–621.10. Kuru B, Gulcelik NE, Gulcelik MA, Dincer H. The false-negative rate of fine-needle aspiration cytology for diagnosing thyroid carcinoma in thyroid nodules. Langenbecks Arch Surg. 2010; 395:127–132.11. Rosario PW, Salles DS, Bessa B, Purisch S. Low false-negative rate of cytology in thyroid nodules >or= 4 cm. Arq Bras Endocrinol Metabol. 2009; 53:1143–1145.12. Raj MD, Grodski S, Woodruff S, Yeung M, Paul E, Serpell JW. Diagnostic lobectomy is not routinely required to exclude malignancy in thyroid nodules greater than four centimetres. ANZ J Surg. 2012; 82:73–77.13. Shrestha M, Crothers BA, Burch HB. The impact of thyroid nodule size on the risk of malignancy and accuracy of fine-needle aspiration: a 10-year study from a single institution. Thyroid. 2012; 22:1251–1256.14. Papini E, Guglielmi R, Bianchini A, Crescenzi A, Taccogna S, Nardi F, Panunzi C, Rinaldi R, Toscano V, Pacella CM. Risk of malignancy in nonpalpable thyroid nodules: predictive value of ultrasound and color-Doppler features. J Clin Endocrinol Metab. 2002; 87:1941–1946.15. Khoo ML, Asa SL, Witterick IJ, Freeman JL. Thyroid calcification and its association with thyroid carcinoma. Head Neck. 2002; 24:651–655.16. Frates MC, Benson CB, Doubilet PM, Kunreuther E, Contreras M, Cibas ES, Orcutt J, Moore FD Jr, Larsen PR, Marqusee E, Alexander EK. Prevalence and distribution of carcinoma in patients with solitary and multiple thyroid nodules on sonography. J Clin Endocrinol Metab. 2006; 91:3411–3417.17. Alexander EK, Marqusee E, Orcutt J, Benson CB, Frates MC, Doubilet PM, Cibas ES, Atri A. Thyroid nodule shape and prediction of malignancy. Thyroid. 2004; 14:953–958.18. Kwak JY, Kim EK, Kim MJ, Hong SW, Choi SH, Son EJ, Oh KK, Park CS, Chung WY, Kim KW. The role of ultrasound in thyroid nodules with a cytology reading of “suspicious for papillary thyroid carcinoma”. Thyroid. 2008; 18:517–522.19. Moon WJ, Jung SL, Lee JH, Na DG, Baek JH, Lee YH, Kim J, Kim HS, Byun JS, Lee DH. Thyroid Study Group, Korean Society of Neuro- and Head and Neck Radiology. Benign and malignant thyroid nodules: US differentiation: multicenter retrospective study. Radiology. 2008; 247:762–770.20. Wienke JR, Chong WK, Fielding JR, Zou KH, Mittelstaedt CA. Sonographic features of benign thyroid nodules: interobserver reliability and overlap with malignancy. J Ultrasound Med. 2003; 22:1027–1031.21. Iannuccilli JD, Cronan JJ, Monchik JM. Risk for malignancy of thyroid nodules as assessed by sonographic criteria: the need for biopsy. J Ultrasound Med. 2004; 23:1455–1464.22. Cibas ES, Ali SZ. NCI Thyroid FNA State of the Science Conference. The Bethesda system for reporting thyroid cytopathology. Am J Clin Pathol. 2009; 132:658–665.23. Yoon JH, Kwak JY, Moon HJ, Kim MJ, Kim EK. The diagnostic accuracy of ultrasound-guided fine-needle aspiration biopsy and the sonographic differences between benign and malignant thyroid nodules 3 cm or larger. Thyroid. 2011; 21:993–1000.24. Gharib H, Papini E, Valcavi R, Baskin HJ, Crescenzi A, Dottorini ME, Duick DS, Guglielmi R, Hamilton CR Jr, Zeiger MA, Zini M. AACE/AME Task Force on Thyroid Nodules. American Association of Clinical Endocrinologists and Associazione Medici Endocrinologi medical guidelines for clinical practice for the diagnosis and management of thyroid nodules. Endocr Pract. 2006; 12:63–102.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Indications for Fine Needle Aspiration in Thyroid Nodules
- Thyroid nodules with discordant results of ultrasonographic and fine-needle aspiration findings
- Natural Course of Cytologically Diagnosed Benign Thyroid Nodules
- Thyroid Nodules with Nondiagnostic FNA Results: Role of Core Needle Biopsy
- The Impact of Thyroid Nodule Size and Fine-Needle Aspiration Biopsy Result on the Risk of Malignancy in the Patients Who Underwent Thyroidectomy
