Clinical Study on Percutaneous Intramedullary Bioresorbable Pin Fixation for Fourth and Fifth Metacarpal Bone Fracture
- Affiliations
-
- 1Department of Plastic and Reconstructive Surgery, Inha University Hospital, Inha University School of Medicine, Incheon, Korea.
- 2Department of Plastic and Reconstructive Surgery, Soonchunhyang University Bucheon Hospital, Soonchunhyang University College of Medicine, Bucheon, Korea. peunsoo@schmc.ac.kr
- KMID: 2383802
- DOI: http://doi.org/10.12790/jkssh.2017.22.2.105
Abstract
- PURPOSE
Metacarpal fracture of a ring and little finger occurs frequently. Percutaneous intramedullary fixation is a simple and effective method with a low incidence of complications. To date, Kirschner wire (K-wire) fixation has been widely used, but this has problems such as pin infection. Moreover it is difficult to start early active motion exercise. So, we replaced the K-wire with a bioresorbable implant and evaluated the results.
METHODS
This study was conducted from 2014 to 2016 and involved 10 consecutive patients with 10 metacarpal neck fractures. All cases underwent percutaneous intramedullary fixation using the ActivaPin (Bioretec Ltd.) within 7 days after injury, and the average follow-up period was 13 months. At the final follow-up, all cases were assessed in terms of total active motion (TAM), bony union and angular deformity based on plain radiographs.
RESULTS
The patients started active motion exercise within 1 week and regained a full range of motion after average 4 weeks. The TAM results were excellent at 250° to 270° in all cases. Regarding radiographic findings, fractures united in all cases and there were no malunion and knuckle deformity.
CONCLUSION
Replacement of a K-wire with a bioresorbable pin prevented soft tissue damage and dorsal scarring. And our percutaneous intramedullary bioresorbable pin fixation technique resulted in early recovery of range of motion and correction of deformity. The patients regained range of motion and returned to daily life early.
MeSH Terms
Figure
-
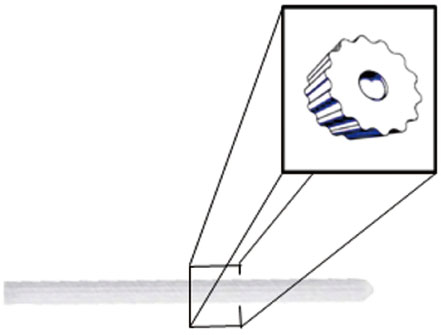
Fig. 1 ActivaPin (2.0 mm×70.0 mm; Bioretec Ltd.) has grooved surface design, and it contributed to a self-locking effect with the adjacent the bone.
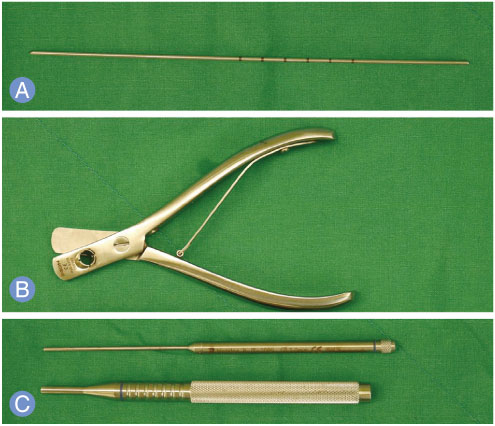
Fig. 2 The ActivaPin (Bioretec Ltd.) device. (A) ActivaPin guide Kirschner wire was used to produce an accurate hole at the site of the ActivaPin. (B) ActivaPin cutter cut the ActivaPin 2 mm shorter than inserted guided pin length. (C) ActivaPin piston (upper) attached ActivaPin and slide inside the ActivaPin sleeve (lower).
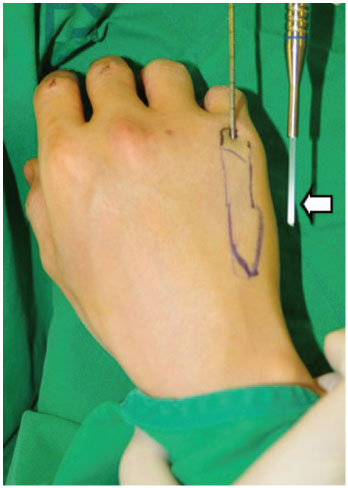
Fig. 3 Intraoperative photograph. To produce an accurate hole where the ActivaPin (arrow; Bioretec Ltd.) is located, a Kirschner wire is inserted percutaneously into the intramedullary canal with flexion of the metacarpophalangeal joint.
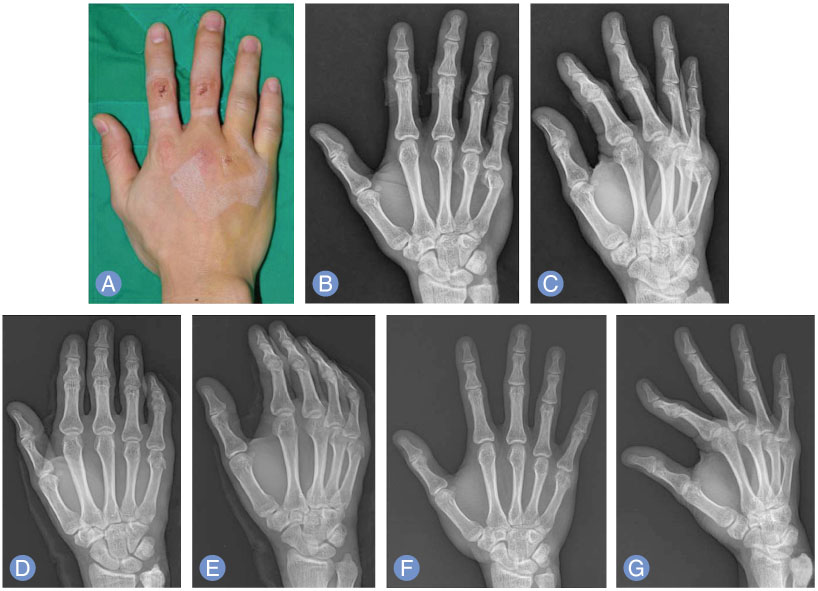
Fig. 4 Preoperative clinical photograph and simple radiograph. (A–C) Preoperative photographic and X-ray findings of a 32-year-old male with a fifth metacarpal neck fracture. (D, E) X-ray at 1 day postoperatively showing a percutaneous intramedullary bioresorbable pin fixation state. (F, G) At 6 months after the operation, radiographs show bony union without dorsal angulation.
Reference
-
1. Chin SH, Vedder NB. MOC-PSSM CME article: metacarpal fractures. Plast Reconstr Surg. 2008; 121:1 Suppl. 1–13.
Article2. Greene TL. Metacarpal fractures. American Society for Surgery of the Hand. Hand surgery update. Rosemonmt, IL: American Academy of Orthopaedic Surgeons;1996. p. 11–15.3. Choi JY, Shin HK, Son KM, Ko CS. Operative treatment in fracture-dislocations of carpometacarpal joints. J Korean Fract Soc. 2005; 18:443–451.
Article4. Low CK, Wong HC, Low YP, Wong HP. A cadaver study of the effects of dorsal angulation and shortening of the metacarpal shaft on the extension and flexion force ratios of the index and little fingers. J Hand Surg Br. 1995; 20:609–613.
Article5. Gonzalez MH, Igram CM, Hall RF Jr. Flexible intramedullary nailing for metacarpal fractures. J Hand Surg Am. 1995; 20:382–387.
Article6. Foucher G. “Bouquet” osteosynthesis in metacarpal neck fractures: a series of 66 patients. J Hand Surg Am. 1995; 20(3 Pt 2):S86–S90.
Article7. Chung NS, Sim JC, Hong KD, Ha SS, Kang JH, Park SJ. Intramedullary pin fixation of metacarpal fractures reduced percutaneously by towel clip. J Korean Soc Surg Hand. 2005; 10:39–44.8. Faraj AA, Davis TR. Percutaneous intramedullary fixation of metacarpal shaft fractures. J Hand Surg Br. 1999; 24:76–79.
Article9. Jahss SA. Fractures of the metacarpals: a new method of reduction and immobilization. J Bone Joint Surg Am. 1938; 20:178–186.10. McCue FC 3rd, Meister K. Common sports hand injuries: an overview of aetiology, management and prevention. Sports Med. 1993; 15:281–289.11. Klein DM, Belsole RJ. Percutaneous treatment of carpal, metacarpal, and phalangeal injuries. Clin Orthop Relat Res. 2000; (375):116–125.
Article12. Theeuwen GA, Lemmens JA, van Niekerk JL. Conservative treatment of boxer’s fracture: a retrospective analysis. Injury. 1991; 22:394–396.
Article13. Black D, Mann RJ, Constine R, Daniels AU. Comparison of internal fixation techniques in metacarpal fractures. J Hand Surg Am. 1985; 10:466–472.
Article14. Fambrough RA, Green DP. Tendon rupture as a complication of screw fixation in fractures in the hand: a case report. J Bone Joint Surg Am. 1979; 61:781–782.
Article15. Stern PJ, Wieser MJ, Reilly DG. Complications of plate fixation in the hand skeleton. Clin Orthop Relat Res. 1987; (214):59–65.
Article16. Lord RE. Intramedullary fixation of metacarpal fractures. J Am Med Assoc. 1957; 164:1746–1749.
Article17. Wong TC, Ip FK, Yeung SH. Comparison between percutaneous transverse fixation and intramedullary K-wires in treating closed fractures of the metacarpal neck of the little finger. J Hand Surg Br. 2006; 31:61–65.
Article18. Choi SJ, Chang SK. Treatment method of the metacarpal bone fractures with retrograde percutaneous intramedullary K-wire fixation to decrease the injury of extensor tendon. J Korean Soc Surg Hand. 2004; 9:117–122.19. Calder JD, O’Leary S, Evans SC. Antegrade intramedullary fixation of displaced fifth metacarpal fractures. Injury. 2000; 31:47–50.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Metacarpal Shaft Fracture Treated by Closed Reduction and Percutaneous Intramedullary K-wire Fixationv
- Surgical Techniques for Percutaneous Reduction by Towel Clips and Percutaneous Intramedullary Fixation with Steinmann Pins for Clavicle Shaft Fractures
- Percutaneous Retrograde Intramedullary Pin Fixation for Isolated Metacarpal Shaft Fracture of the Little Finger
- Bouquet Pin Intramedullary Nail Technique of the 5th Metacarpal Neck Fractures
- Comparison between Intramedullary Nailing and Percutaneous K-Wire Fixation for Fractures in the Distal Third of the Metacarpal Bone
