J Korean Soc Surg Hand.
2017 Jun;22(2):96-104. 10.12790/jkssh.2017.22.2.96.
Double Minimal Incision Release for Carpal Tunnel Syndrome: A Comparative Study to the Standard Open Technique
- Affiliations
-
- 1Department of Orthopedic Surgery, Inha University School of Medicine, Incheon, Korea. TJLEE@inha.ac.kr
- KMID: 2383801
- DOI: http://doi.org/10.12790/jkssh.2017.22.2.96
Abstract
- PURPOSE
A minimally invasive surgical technique has been introduced to treat carpal tunnel syndrome that causes less pain, minimal scaring, and a rapid recovery. This study was designed to evaluate the safety and effectiveness of the double minimal incision release compared with the open surgery technique.
METHODS
A study was performed on 175 cases in 111 patients who were operated on for carpal tunnel syndrome from January 2010 to December 2014. The patients were classified into 2 groups according to the type of surgical technique: 82 cases underwent standard open surgery in group A and 93 cases underwent double minimal incision release in group B. Grip strength and postoperative pain were evaluated 4 and 8 weeks and 6 and 12 months after surgery, and the period of numbness and time needed to resume normal activities were investigated.
RESULTS
Group B patients showed better outcomes during the 2 first months after surgery than those of group A patients in numbness, pain, stiffness (p<0.05), less scar pain and tenderness (p<0.001), and shorter time needed to resume normal activities. However, no differences in these parameters were observed between the 2 groups after 6 months (p>0.05).
CONCLUSION
Double minimal incision release offered better clinical outcomes until 2 months after surgery compared to the standard open surgery technique and reduced incipient postoperative pain and allowed for earlier resumption of normal activities.
MeSH Terms
Figure
-

Fig. 1 Measurement of pillar tenderness.

Fig. 2 Skin incision of standard open technique.

Fig. 3 Skin incision of double minimal incision technique. A 1-cm distal incision (A) was made longitudinally along the proximal portion of median crease to expose the distal margin of the transverse carpal ligament, which was divided under direct vision. And a 1-cm incision (B) was made transversely at the wrist crease over the palmaris longus tendon.
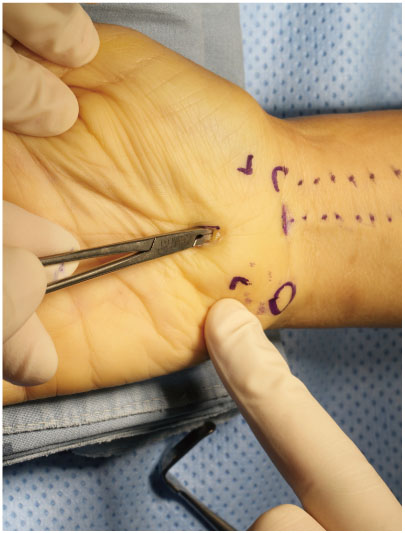
Fig. 4 Confirmation of complete release of transverse carpal ligament with curved mosquito forceps.
Reference
-
1. Brown RA, Gelberman RH, Seiler JG 3rd, et al. Carpal tunnel release: a prospective, randomized assessment of open and endoscopic methods. J Bone Joint Surg Am. 1993; 75:1265–1275.
Article2. Phalen GS. The carpal-tunnel syndrome: seventeen years’ experience in diagnosis and treatment of six hundred fifty-four hands. J Bone Joint Surg Am. 1966; 48:211–228.3. Kulick MI, Gordillo G, Javidi T, Kilgore ES Jr, Newmayer WL 3rd. Long-term analysis of patients having surgical treatment for carpal tunnel syndrome. J Hand Surg Am. 1986; 11:59–66.
Article4. Kuschner SH, Brien WW, Johnson D, Gellman H. Complications associated with carpal tunnel release. Orthop Rev. 1991; 20:346–352.5. Seiler JG 3rd, Barnes K, Gelberman R. Endoscopic carpal tunnel release: an anatomic study of the two-incision method in human cadavers. J Hand Surg Am. 1992; 17:996–1002.
Article6. Seradge H, Seradge E. Piso-triquetral pain syndrome after carpal tunnel release. J Hand Surg Am. 1989; 14:858–862.
Article7. MacDonald RI, Lichtman DM, Hanlon JJ, Wilson JN. Complications of surgical release for carpal tunnel syndrome. J Hand Surg Am. 1978; 3:70–76.
Article8. Elsharif M, Papanna M, Helm R. Long-term follow up outcome results of Knifelight carpal tunnel release and conventional open release following a departmental randomized controlled trial: a prospective study. Pol Orthop Traumatol. 2014; 79:67–70.9. Nazzi V, Franzini A, Messina G, Broggi G. Carpal tunnel syndrome: matching minimally invasive surgical techniques: technical note. J Neurosurg. 2008; 108:1033–1036.10. Agee JM, Peimer CA, Pyrek JD, Walsh WE. Endoscopic carpal tunnel release: a prospective study of complications and surgical experience. J Hand Surg Am. 1995; 20:165–171.
Article11. Taleisnik J. The palmar cutaneous branch of the median nerve and the approach to the carpal tunnel: an anatomical study. J Bone Joint Surg Am. 1973; 55:1212–1217.12. Chow JC. Endoscopic release of the carpal ligament: a new technique for carpal tunnel syndrome. Arthroscopy. 1989; 5:19–24.
Article13. Trumble TE, Diao E, Abrams RA, Gilbert-Anderson MM. Single-portal endoscopic carpal tunnel release compared with open release: a prospective, randomized trial. J Bone Joint Surg Am. 2002; 84:1107–1115.14. Macdermid JC, Richards RS, Roth JH, Ross DC, King GJ. Endoscopic versus open carpal tunnel release: a randomized trial. J Hand Surg Am. 2003; 28:475–480.
Article15. Masear VR, Hayes JM, Hyde AG. An industrial cause of carpal tunnel syndrome. J Hand Surg Am. 1986; 11:222–227.
Article16. Chow JC. Endoscopic release of the carpal ligament for carpal tunnel syndrome: 22-month clinical result. Arthroscopy. 1990; 6:288–296.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Double Incision Technique for Carpal Tunnel Release
- Comparison of Clinical Results of Minimal Incision Versus Endoscopic Carpal Tunnel Release
- Limited Two Incision Technique in Carpal Tunnel Release
- Clinical Results of Open versus Endoscopic Carpal Tunnel Release
- The Efficacy of Carpal Tunnel Release with Mini-Open Incision
