Endoscopic Resection of a Giant Esophageal Lipoma Causing Sudden Choking
- Affiliations
-
- 1Department of Internal Medicine, Wonkwang University College of Medicine, Iksan, Korea. jipsinsa@naver.com
- KMID: 2383517
- DOI: http://doi.org/10.4166/kjg.2016.68.4.210
Abstract
- Most esophageal lipomas are discovered incidentally and are small and asymptomatic. However, large (>4 cm) lipomas may cause various symptoms, including dysphagia, regurgitation, or epigastric discomfort. We present a 45-year-old woman with intermittent sudden choking and globus pharyngeus. Upper gastrointestinal endoscopy and endoscopic ultrasound revealed an approximately 10.0×1.5 cm pedunculated subepithelial tumor in the upper esophagus, identified as the cause of her symptoms. A thoracic computed tomography scan revealed a fat attenuated longitudinal mass along the upper esophagus, suggestive of a lipoma. Endoscopic resection of the lesion was performed with a detachable snare to relieve her symptoms, and the pathologic findings were consistent with a lipoma.
MeSH Terms
Figure
-
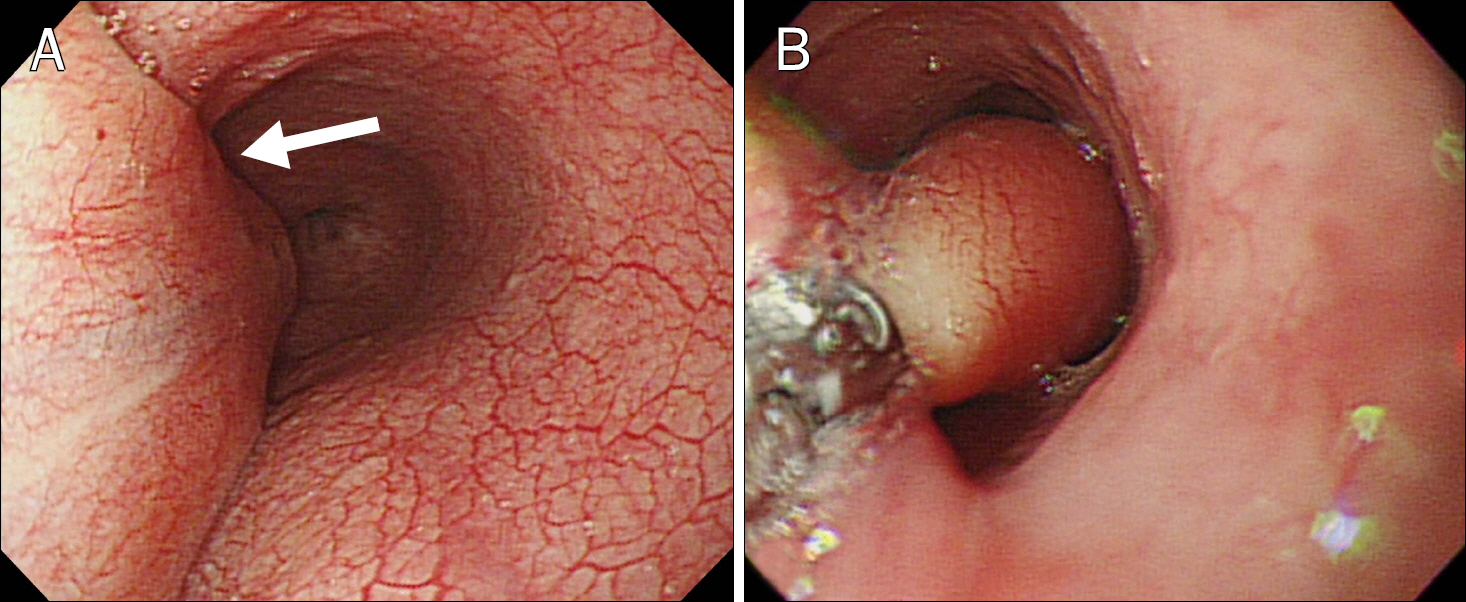
Fig. 1. (A) Endoscopic images showing a pedunculated subepithelial tumor with a large pedicle covered with normal mucosa originating in the cervical esophagus (arrow). (B) Positive “pillow sign” and the yellowish, smooth mucosal surface are visible.
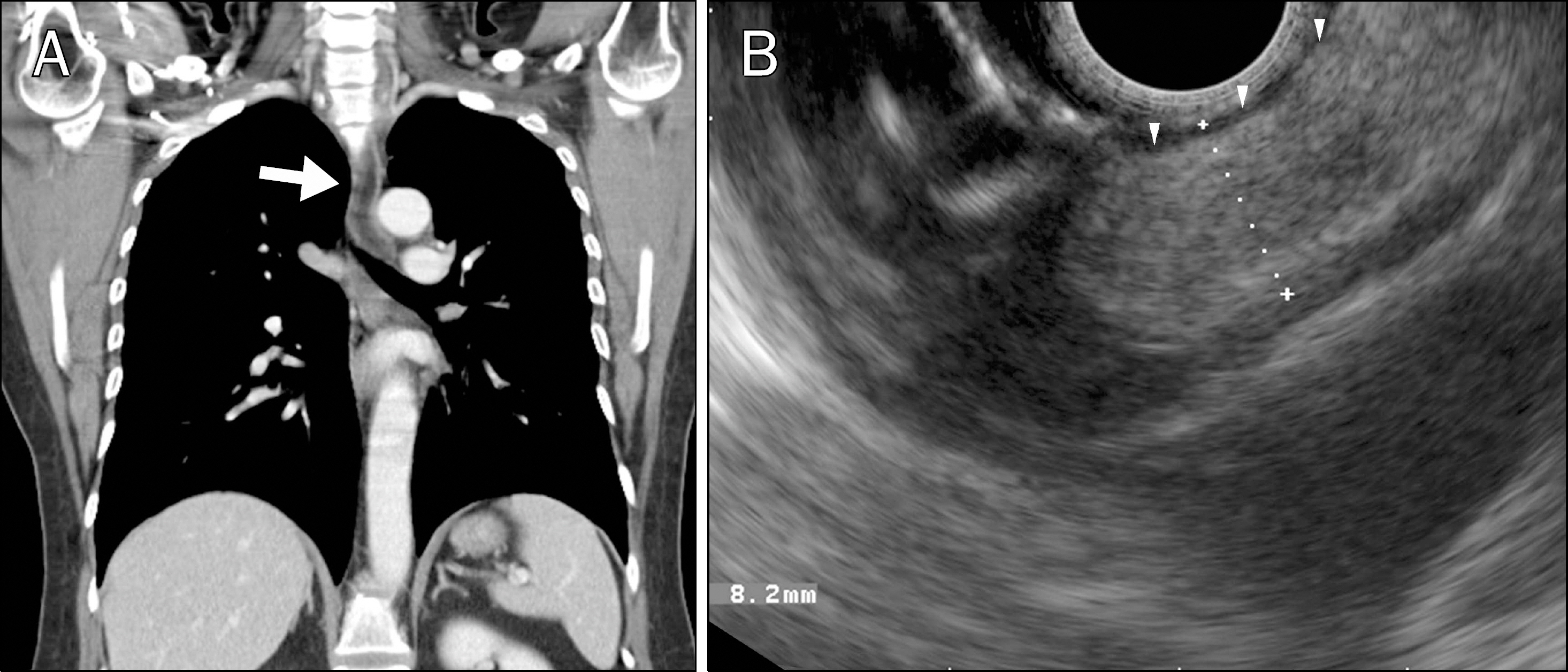
Fig. 2. (A) Thoracic computed tomography scan showing a longitudinal mass with fat density (arrow), elongated approximately 8 cm along the upper esophagus. (B) Endoscopic ultrasound showing a hyperechoic lesion with a smooth margin arising from the submucosal layer of the esophagus (arrowheads).

Fig. 3. (A) The placement of a detachable snare around the thick stalk of the esophageal subepithelial tumor. (B) Resection defect after removal of the subepithelial tumor using the standard diathermy snare.
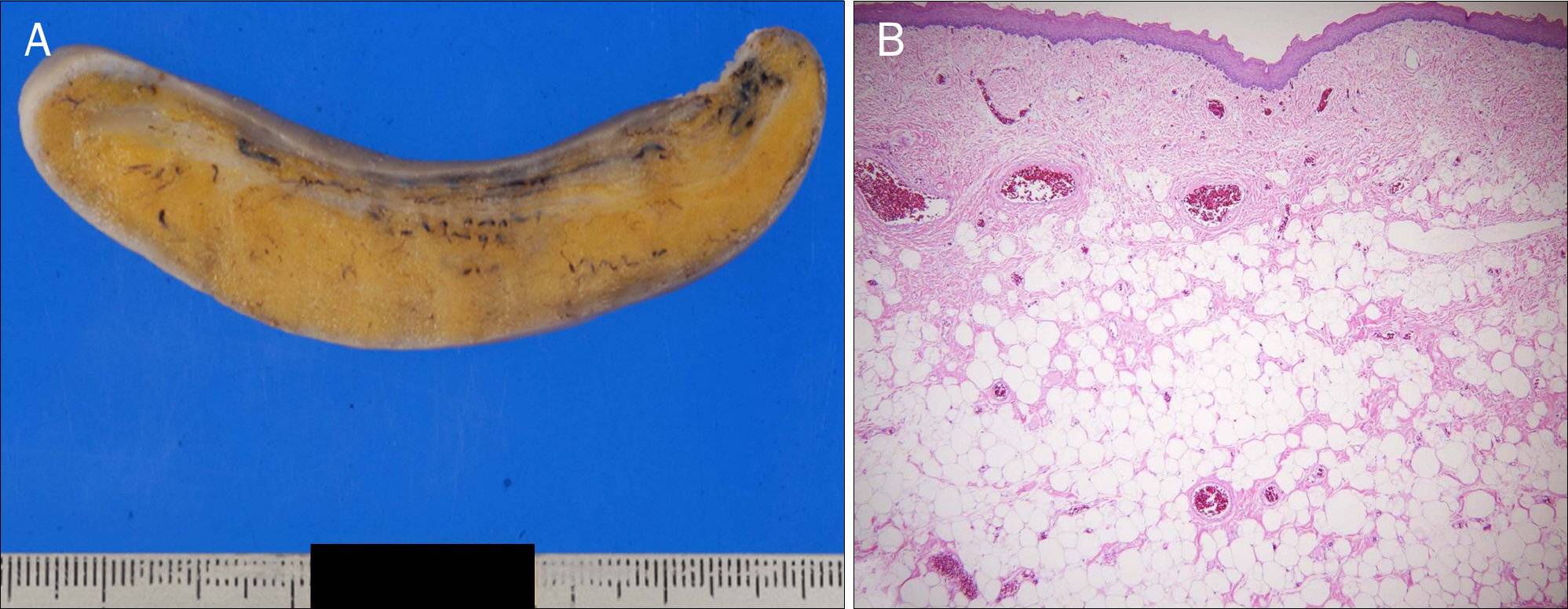
Fig. 4. (A) Gross finding of the cut surface demonstrating a smooth and yellowish shaped mass, similar to a banana. (B) Histologic examination showing lobules of mature adipocytes, consistent with lipoma (H&E, ×40).
Reference
-
References
1. Kang JY, Chan-Wilde C, Wee A, Chew R, Ti TK. Role of computed tomography and endoscopy in the management of alimentary tract lipomas. Gut. 1990; 31:550–553.
Article2. Feldman J, Tejerina M, Hallowell M. Esophageal lipoma: a rare tumor. J Radiol Case Rep. 2012; 6:17–22.
Article3. Cochet B, Hohl P, Sans M, Cox JN. Asphyxia caused by laryngeal impaction of an esophageal polyp. Arch Otolaryngol. 1980; 106:176–178.
Article4. Allen MS Jr, Talbot WH. Sudden death due to regurgitation of a pedunculated esophageal lipoma. J Thorac Cardiovasc Surg. 1967; 54:756–758.5. Hurwitz MM, Redleaf PD, Williams HJ, Edwards JE. Lipomas of the gastrointestinal tract. An analysis of seventy-two tumors. Am J Roentgenol Radium Ther Nucl Med. 1967; 99:84–89.6. Chung JJ, Kim MJ, Kim JH, Lee JT, Yoo HS, Kim KW. Imaging findings of giant liposarcoma of the esophagus. Yonsei Med J. 2003; 44:715–718.
Article7. Bhatia V, Tajika M, Rastogi A. Upper gastrointestinal submucosal lesions–clinical and endosonographic evaluation and management. Trop Gastroenterol. 2010; 31:5–29.8. Medici JR, Gomez NL, Wright FG, et al. Giant esophageal lipoma. J Gastrointest Surg. 2016; 20:473–475.
Article9. Cheriyan D, Guy C, Burbridge R. Giant esophageal lipoma: endoscopic resection. Gastrointest Endosc. 2015; 82:742.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Giant Colonic Lipoma Showing Spontaneous Resolution after Endoscopic Partial Resection
- A Case of a Colonic Giant Lipoma Removed by Endoscopic Resection
- Case of a Giant Colonic Lipoma That Was Endoscopically Removed by Strangulation with Repetitive Endoloop Ligation
- Choking by Esophageal Foreign Body Impaction
- Endoscopic Resection of Giant Colonic Lipoma: Case Series with Partial Resection
