Clin Endosc.
2016 Nov;49(6):560-563. 10.5946/ce.2016.048.
An Intractable Caustic Esophageal Stricture Successfully Managed with Sequential Treatment Comprising Incision with an Insulated-Tip Knife, Balloon Dilation, and an Oral Steroid
- Affiliations
-
- 1Division of Gastroenterology, Department of Internal Medicine, Presbyterian Medical Center, Jeonju, Korea. jeja-1004@daum.net
- KMID: 2383453
- DOI: http://doi.org/10.5946/ce.2016.048
Abstract
- Bougie or balloon dilation is a good short-term treatment for caustic esophageal strictures, although recurrence after dilation occurs in approximately 30% of these cases. Therefore, long-term treatment options are required in some cases, and endoscopic incisional therapy has been used for patients with an anastomotic stricture in the gastrointestinal tract. A 58-year-old woman presented with severe swallowing difficulty because of a caustic esophageal stricture, which was caused by accidental exposure to anhydrous acetic acid at infancy. She had undergone several previous bougie and balloon dilations but the stricture did not improve. We performed sequential treatment comprising incision with an insulated-tip knife, balloon dilation, and an oral steroid, which resulted in the patient's symptoms markedly improving. Thus, we report this case of an intractable caustic esophageal stricture, which was successfully treated using combined endoscopic sequential treatment.
MeSH Terms
Figure
-
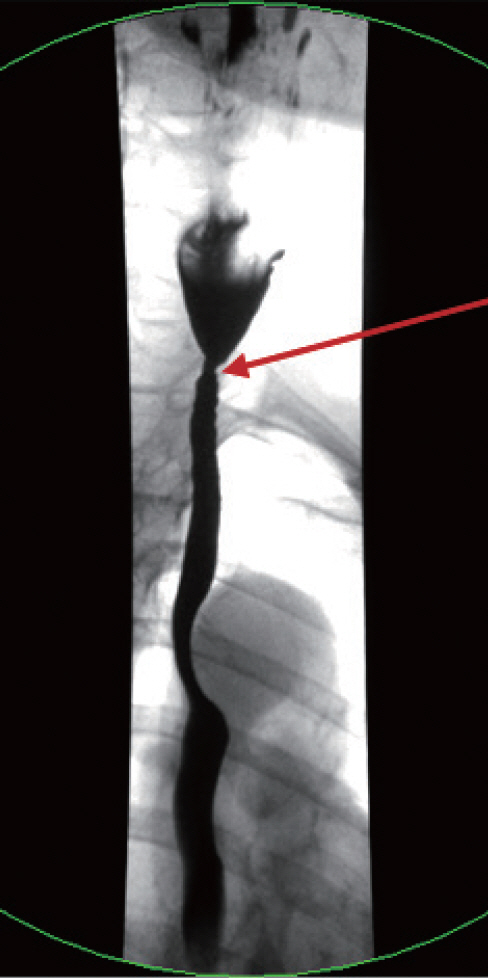
Fig. 1. The esophageal stricture was located 18 cm from the incisor.
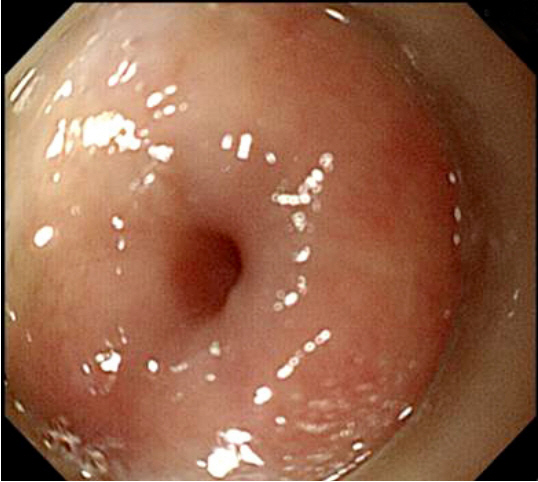
Fig. 2. Endoscopy reveals a severe stricture in the cervical esophagus.

Fig. 3. Fluoroscopic imaging of an unsuccessful attempt to use balloon dilation to treat the narrowed segment.
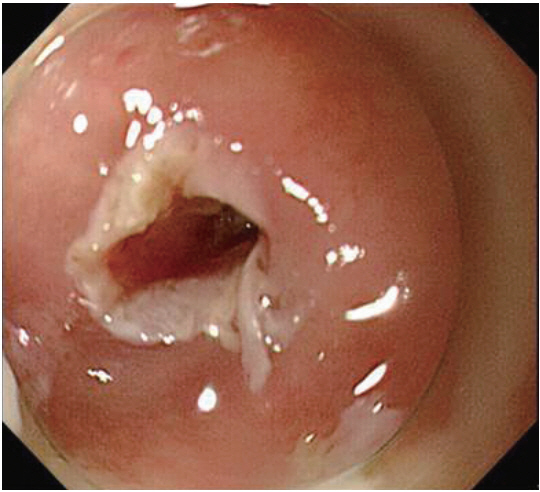
Fig. 4. Incisional therapy using an insulated-tip electrosurgical knife.
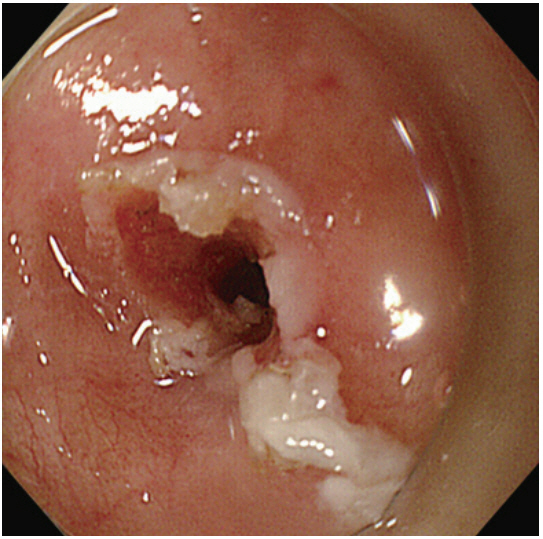
Fig. 5. Endoscopy immediately after the incisional therapy reveals marked improvement at the stricture.
Reference
-
1. Pereira-Lima JC, Ramires RP, Zamin I Jr, Cassal AP, Marroni CA, Mattos AA. Endoscopic dilation of benign esophageal strictures: report on 1043 procedures. Am J Gastroenterol. 1999; 94:1497–1501.
Article2. Scolapio JS, Pasha TM, Gostout CJ, et al. A randomized prospective study comparing rigid to balloon dilators for benign esophageal strictures and rings. Gastrointest Endosc. 1999; 50:13–17.
Article3. Patterson DJ, Graham DY, Smith JL, et al. Natural history of benign esophageal stricture treated by dilatation. Gastroenterology. 1983; 85:346–350.
Article4. Saeed ZA, Ramirez FC, Hepps KS, et al. An objective end point for dilation improves outcome of peptic esophageal strictures: a prospective randomized trial. Gastrointest Endosc. 1997; 45:354–359.
Article5. ASGE Technology Committee, Siddiqui UD, Banerjee S, et al. Tools for endoscopic stricture dilation. Gastrointest Endosc. 2013; 78:391–404.
Article6. Canhoto M, Arroja B, Silva F, Gonçalves C, Cotrim I, Vasconcelos H. Needle-knife incisional treatment of refractory esophagic caustic stenosis. Endoscopy. 2011; 43 Suppl 2 UCTN:E386.
Article7. Coia LR, Myerson RJ, Tepper JE. Late effects of radiation therapy on the gastrointestinal tract. Int J Radiat Oncol Biol Phys. 1995; 31:1213–1236.
Article8. Zargar SA, Kochhar R, Nagi B, Mehta S, Mehta SK. Ingestion of strong corrosive alkalis: spectrum of injury to upper gastrointestinal tract and natural history. Am J Gastroenterol. 1992; 87:337–341.9. Mills LJ, Estrera AS, Platt MR. Avoidance of esophageal stricture following severe caustic burns by the use of an intraluminal stent. Ann Thorac Surg. 1979; 28:60–65.
Article10. Da-Costa-Pinto EA, Dorsa TK, Altimani A, et al. A functional study of caustic strictures of the esophagus in children. Braz J Med Biol Res. 2004; 37:1623–1630.
Article11. van Boeckel PG, Siersema PD. Refractory esophageal strictures: what to do when dilation fails. Curr Treat Options Gastroenterol. 2015; 13:47–58.
Article12. Lew RJ, Kochman ML. A review of endoscopic methods of esophageal dilation. J Clin Gastroenterol. 2002; 35:117–126.
Article13. Kochman ML, McClave SA, Boyce HW. The refractory and the recurrent esophageal stricture: a definition. Gastrointest Endosc. 2005; 62:474–475.
Article14. Samanta J, Dhaka N, Sinha SK, Kochhar R. Endoscopic incisional therapy for benign esophageal strictures: Technique and results. World J Gastrointest Endosc. 2015; 7:1318–1326.
Article15. Hordijk ML, van Hooft JE, Hansen BE, Fockens P, Kuipers EJ. A randomized comparison of electrocautery incision with Savary bougienage for relief of anastomotic gastroesophageal strictures. Gastrointest Endosc. 2009; 70:849–855.
Article16. Moretó M, Zaballa M, Ibáñez S. Endoscopic incision as an alternative to bougienage in the treatment of peptic esophageal stricture. Endoscopy. 1990; 22:105–109.
Article17. Wills JC, Hilden K, Disario JA, Fang JC. A randomized, prospective trial of electrosurgical incision followed by rabeprazole versus bougie dilation followed by rabeprazole of symptomatic esophageal (Schatzki’s) rings. Gastrointest Endosc. 2008; 67:808–813.
Article18. Hagiwara A, Togawa T, Yamasaki J, Shirasu M, Sakakura C, Yamagishi H. Endoscopic incision and balloon dilatation for cicatricial anastomotic strictures. Hepatogastroenterology. 1999; 46:997–999.19. Kochhar R, Makharia GK. Usefulness of intralesional triamcinolone in treatment of benign esophageal strictures. Gastrointest Endosc. 2002; 56:829–834.
Article20. Kim GH, Jee SR, Jang JY, et al. Stricture occurring after endoscopic submucosal dissection for esophageal and gastric tumors. Clin Endosc. 2014; 47:516–522.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- High grade anorectal stricture complicating Crohn's disease: endoscopic treatment using insulated-tip knife
- The Role of Endoscopic Balloon Dilation in the Treatment of Esophageal Strictures
- Stent Flange-Induced Esophageal Stricture Treated with an Oral Steroid
- Use of an insulated tip knife in the management of a common foreign body in a child
- Caustic Esophagitis and Gastrofiberoscopy in Children
