Intrahepatic Cholangiocarcinoma with Ductal Plate Malformation-like Feature Associated with Bile Duct Adenoma
- Affiliations
-
- 1Department of Pathology, CHA Bundang Medical Center, CHA University, Seongnam, Korea. blacknw@cha.ac.kr
- KMID: 2381413
- DOI: http://doi.org/10.4132/jptm.2015.06.19
Abstract
- No abstract available.
Figure
-
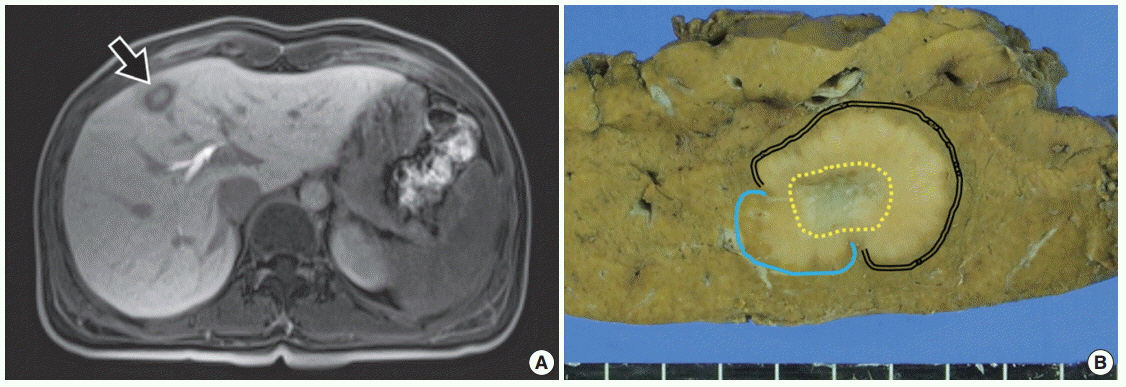
Fig. 1. Radiologic and gross findings. (A) Magnetic resonance imaging of the liver reveals a 2-cm target appearance lesion (arrow) in segment 4. On a T1-weighted image, the central portion shows low signal intensity (SI), and the peripheral zone shows intermediate to slightly high SI. (B) Grossly, the tumor is a relatively well-defined, solid, pale brown mass with a multinodular margin and central fibrous scar. The tumor has three areas: double line of right upper area, cholangiocarcinoma; dotted central circle, dilated ducts with fibrous stroma; and line of left lower area, bile duct adenoma.

Fig. 2. Microscopic findings of the tumor. (A) One peripheral portion shows highly packed ducts with bland looking nuclei; bile duct adenoma containing portal tracts (arrow). (B) Central area reveals irregularly dilated glandular structures within fibrous stroma, resembling features of ductal plate malformation. (C) In the other peripheral lesion, fused and cribriform glands infiltrate into the stroma. The nuclei are atypical and show brisk mitotic activity; cholangiocarcinoma. (D) The tumor shows a transitional area between bile duct adenoma (right) and cholangiocarcinoma(left). Bland uniform ductal structures become irregular and anastomosing.
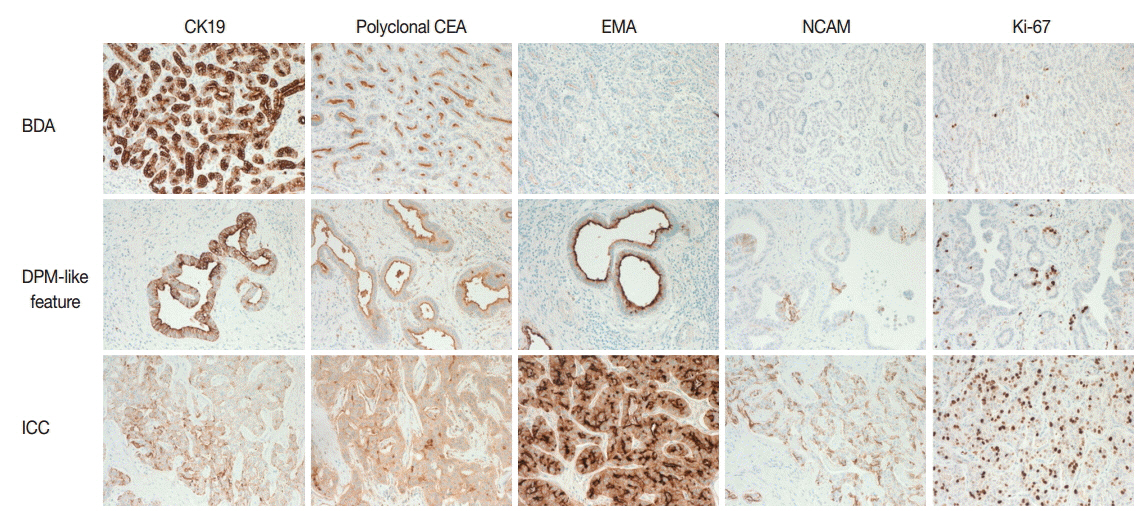
Fig. 3. Immunohistochemical staining patterns in three areas. Cytokerain 19 (CK19) and polyclonal carcinoembryonic antigen (CEA) are positive in all areas, but intensity and location are different. Epithelial membrane antigen (EMA) and NCAM are negative in the bile duct adenoma (BDA) area, weakly positive in the ductal plate malformation (DPM) area, and positive in the cholangiocarcinoma (ICC) area. The Ki-67 labeling index differs in the different areas, from 1%–2% in BDA to 40%–50% in the cholangiocarcinoma area.
Reference
-
1. Jain D, Nayak NC, Saigal S. Hepatocellular carcinoma arising in association with von-Meyenburg’s complexes: an incidental finding or precursor lesions? A clinicopatholigic study of 4 cases. Ann Diagn Pathol. 2010; 14:317–20.
Article2. Xu AM, Xian ZH, Zhang SH, Chen XF. Intrahepatic cholangiocarcinoma arising in multiple bile duct hamartomas: report of two cases and review of the literature. Eur J Gastroenterol Hepatol. 2009; 21:580–4.
Article3. Nakanuma Y, Sato Y, Ikeda H, et al. Intrahepatic cholangiocarcinoma with predominant “ductal plate malformation” pattern: a new subtype. Am J Surg Pathol. 2012; 36:1629–35.4. Nakanuma Y, Tsutsui A, Ren XS, Harada K, Sato Y, Sasaki M. What are the precursor and early lesions of peripheral intrahepatic cholangiocarcinoma? Int J Hepatol. 2014; 2014:805973.
Article5. Terada T. Combined hepatocellular-cholangiocarcinoma with stem cell features, ductal plate malformation subtype: a case report and proposal of a new subtype. Int J Clin Exp Pathol. 2013; 6:737–48.6. Lindgren AG, Hansson G, Nilsson LA. Primary carcinoma arising in congenital liver in conjunction with miliary cholangiomatosis: report of case. Acta Pathol Microbiol Scand. 1961; 52:343–8.7. Desmet VJ. Ductal plates in hepatic ductular reactions. Hypothesis and implications. III. Implications for liver pathology. Virchows Arch. 2011; 458:271–9.
Article8. Hasebe T, Sakamoto M, Mukai K, et al. Cholangiocarcinoma arising in bile duct adenoma with focal area of bile duct hamartoma. Virchows Arch. 1995; 426:209–13.
Article9. Pinho AC, Melo RB, Oliveira M, et al. Adenoma-carcinoma sequence in intrahepatic cholangiocarcinoma. Int J Surg Case Rep. 2012; 3:131–3.
Article10. Takahashi S, Takada K, Kawano Y, et al. Cholangiocarcinoma with bile duct adenoma and hamartoma-like lesion in the bile duct. Nihon Shokakibyo Gakkai Zasshi. 2010; 107:461–9.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Histopathology of a benign bile duct lesion in the liver: Morphologic mimicker or precursor of intrahepatic cholangiocarcinoma
- Intrahepatic cholangiocarcinoma with predominant ductal plate malformation pattern
- Development of Intrahepatic Bile Duct in Human Embryos and Fetuses; Histologic and Immunohfstochemical Observations
- Intrahepatic cholangiocarcinoma presenting as liver Abscess: Report of Two Cases
- RE: Diffusion-Weighted MRI in Intrahepatic Bile Duct Adenoma Arising from the Cirrhotic Liver
