Clinical Outcome of Relapsed or Refractory Burkitt Lymphoma and Mature B-Cell Lymphoblastic Leukemia in Children and Adolescents
- Affiliations
-
- 1Department of Pediatrics, SMG-SNU Boramae Medical Center, Seoul National University College of Medicine, Seoul, Korea.
- 2Department of Pediatrics, Gyeongsang National University School of Medicine, Jinju, Korea. espark@gsnu.ac.kr
- 3Gyeongsang Institute of Health Sciences, Gyeongsang National University, Jinju, Korea.
- 4Department of Pediatrics, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 5Department of Pediatrics, Yonsei University College of Medicine, Seoul, Korea.
- 6Department of Pediatrics, Pusan National University School of Medicine, Busan, Korea.
- 7Department of Pediatrics, Chonnam National University Hwasun Hospital, Chonnam National University Medical School, Hwasun, Korea.
- 8Department of Pediatrics, Seoul National University College of Medicine, Seoul, Korea.
- 9Cancer Research Institute Seoul National University, Seoul, Korea.
- KMID: 2380373
- DOI: http://doi.org/10.4143/crt.2013.047
Abstract
- PURPOSE
Despite the rapid improvement in survival rate from Burkitt lymphoma and mature B-cell lymphoblastic leukemia (B-ALL) in children, a small subset of patients do not respond to first-line chemotherapy or experience relapse (RL). Herein, we report the clinical characteristics and outcomes of these patients.
MATERIALS AND METHODS
RL or refractory Burkitt lymphoma and mature B-ALL in 125 patients diagnosed from 1990 to 2009 were retrospectively analyzed.
RESULTS
Nineteen patients experienced RL or progressive disease (PD). Among them, 12 patients had PD or RL less than six months after initial treatment and seven had late RL. Seven patients achieved complete response (CR), 11 had PD, and one had no more therapy. Six patients who achieved CR survived without evidence of disease and four of them underwent high-dose chemotherapy (HDC) followed by stem cell transplantation (SCT). However, 11 patients who failed to obtain CR eventually died of their disease. Five-year overall survival (OS) was 31.6+/-10.7%. OS of patients with late RL was superior to that of patients with early RL (57.1+/-18.7%, vs. 16.7+/-10.8%, p=0.014). Achievement of CR after reinduction had significant OS (p < 0.001). OS for patients who were transplanted was superior (p < 0.01). In multivariate analysis, achievement of CR after reinduction chemotherapy showed an association with improved OS (p=0.05).
CONCLUSION
Late RL and chemotherapy-sensitive patients have the chance to achieve continuous CR using HDC/SCT, whereas patients who are refractory to retrieval therapy have poor prognosis. Therefore, novel salvage strategy is required for improvement of survival for this small set of patients.
Keyword
MeSH Terms
Figure
-
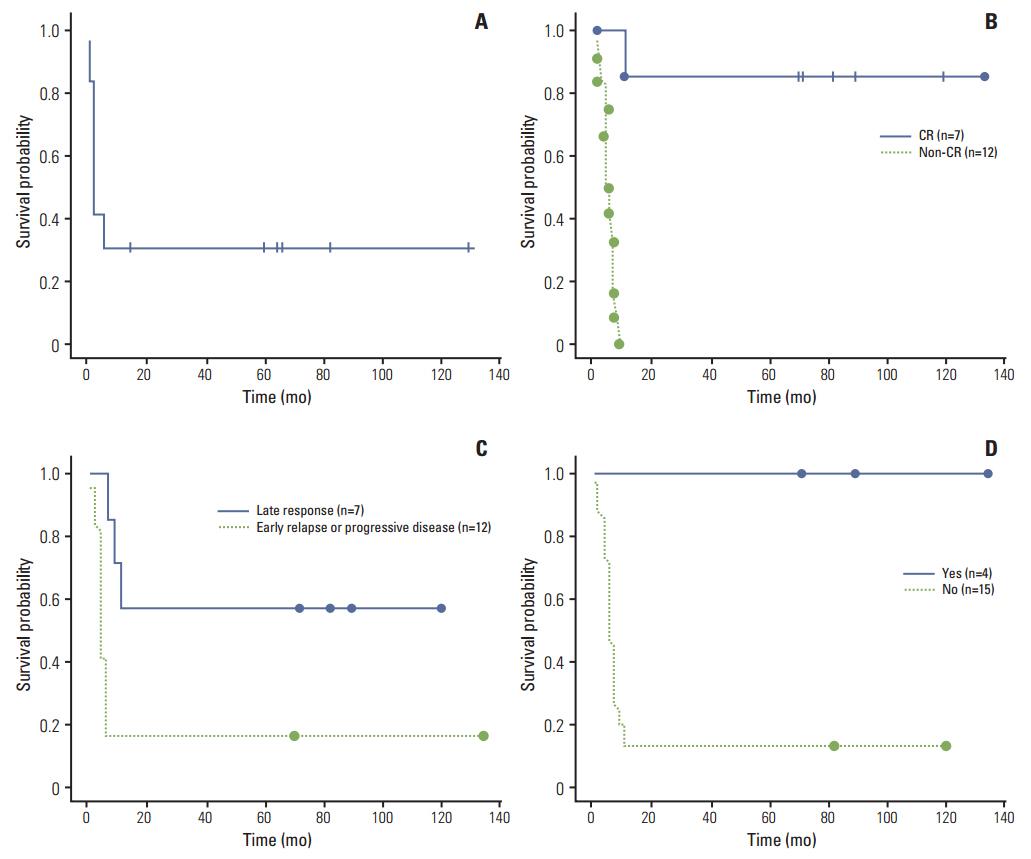
Fig. 1. (A) Overall survival of relapsed or primary refractory disease. Median survival was seven months (95% confidence interval [CI], 5.6 to 8.4). (B) Overall survival of patients who achieved complete response (CR) and non-CR to reinduction chemotherapy, which is statistically significant (p < 0.001). Median survival was 5.5 months (95% CI, 3.4 to 6.6) for patients who had non-CR. (C) Overall survival and time to relapse. Median survival was five months for patients who had primary refractory or early relapse. Survival rate for primary refractory or early relapse and late relapse was 16.7±10.8% and 57.1±18.7, respectively (p < 0.05). (D) Overall survival and hematopoietic stem cell transplantation. Median survival was 6.5 months (95% CI, 4.6 to 8.4) for patients who were not transplanted. Overall survival of both groups was statistically significant (p < 0.01).
Cited by 1 articles
-
Clinical Characteristics and Treatment Outcomes of Pediatric Patients with Non-Hodgkin Lymphoma in East Asia
Jin Kyung Suh, Yi-Jin Gao, Jing-Yan Tang, Shiann-Tarng Jou, Dong-Tsamn Lin, Yoshiyuki Takahashi, Seiji Kojima, Ling Jin, Yonghong Zhang, Jong Jin Seo
Cancer Res Treat. 2020;52(2):359-368. doi: 10.4143/crt.2019.219.
Reference
-
References
1. Patte C, Auperin A, Michon J, Behrendt H, Leverger G, Frappaz D, et al. The Societe Francaise d’Oncologie Pediatrique LMB89 protocol: highly effective multiagent chemotherapy tailored to the tumor burden and initial response in 561 unselected children with B-cell lymphomas and L3 leukemia. Blood. 2001; 97:3370–9.
Article2. Atra A, Imeson JD, Hobson R, Gerrard M, Hann IM, Eden OB, et al. Improved outcome in children with advanced stage B-cell non-Hodgkin’s lymphoma (B-NHL): results of the United Kingdom Children Cancer Study Group (UKCCSG) 9002 protocol. Br J Cancer. 2000; 82:1396–402.
Article3. Patte C, Philip T, Rodary C, Zucker JM, Behrendt H, Gentet JC, et al. High survival rate in advanced-stage B-cell lymphomas and leukemias without CNS involvement with a short intensive polychemotherapy: results from the French Pediatric Oncology Society of a randomized trial of 216 children. J Clin Oncol. 1991; 9:123–32.
Article4. Reiter A, Schrappe M, Tiemann M, Ludwig WD, Yakisan E, Zimmermann M, et al. Improved treatment results in childhood B-cell neoplasms with tailored intensification of therapy: a report of the Berlin-Frankfurt-Munster Group Trial NHL-BFM 90. Blood. 1999; 94:3294–306.5. Cairo MS, Gerrard M, Sposto R, Auperin A, Pinkerton CR, Michon J, et al. Results of a randomized international study of high-risk central nervous system B non-Hodgkin lymphoma and B acute lymphoblastic leukemia in children and adolescents. Blood. 2007; 109:2736–43.
Article6. Philip T, Hartmann O, Pinkerton R, Zucker JM, Gentet JC, Lamagnere JP, et al. Curability of relapsed childhood B-cell non-Hodgkin’s lymphoma after intensive first line therapy: a report from the Societe Francaise d’Oncologie Pediatrique. Blood. 1993; 81:2003–6.
Article7. Atra A, Gerrard M, Hobson R, Imeson JD, Hann IM, Pinkerton CR. Outcome of relapsed or refractory childhood B-cell acute lymphoblastic leukaemia and B-cell non-Hodgkin’s lymphoma treated with the UKCCSG 9003/9002 protocols. Br J Haematol. 2001; 112:965–8.
Article8. Fujita N, Mori T, Mitsui T, Inada H, Horibe K, Tsurusawa M, et al. The role of hematopoietic stem cell transplantation with relapsed or primary refractory childhood B-cell non-Hodgkin lymphoma and mature B-cell leukemia: a retrospective analysis of enrolled cases in Japan. Pediatr Blood Cancer. 2008; 51:188–92.
Article9. Kobrinsky NL, Sposto R, Shah NR, Anderson JR, DeLaat C, Morse M, et al. Outcomes of treatment of children and adolescents with recurrent non-Hodgkin’s lymphoma and Hodgkin’s disease with dexamethasone, etoposide, cisplatin, cytarabine, and l-asparaginase, maintenance chemotherapy, and transplantation: Children’s Cancer Group Study CCG-5912. J Clin Oncol. 2001; 19:2390–6.
Article10. Kung FH, Harris MB, Krischer JP. Ifosfamide/carboplatin/etoposide (ICE), an effective salvaging therapy for recurrent malignant non-Hodgkin lymphoma of childhood: a Pediatric Oncology Group phase II study. Med Pediatr Oncol. 1999; 32:225–6.
Article11. Ladenstein R, Pearce R, Hartmann O, Patte C, Goldstone T, Philip T. High-dose chemotherapy with autologous bone marrow rescue in children with poor-risk Burkitt’s lymphoma: a report from the European Lymphoma Bone Marrow Transplantation Registry. Blood. 1997; 90:2921–30.
Article12. Attarbaschi A, Dworzak M, Steiner M, Urban C, Fink FM, Reiter A, et al. Outcome of children with primary resistant or relapsed non-Hodgkin lymphoma and mature B-cell leukemia after intensive first-line treatment: a population-based analysis of the Austrian Cooperative Study Group. Pediatr Blood Cancer. 2005; 44:70–6.
Article13. Cheson BD, Horning SJ, Coiffier B, Shipp MA, Fisher RI, Connors JM, et al. Report of an international workshop to standardize response criteria for non-Hodgkin’s lymphomas. NCI Sponsored International Working Group. J Clin Oncol. 1999; 17:1244.14. Gerrard M, Cairo MS, Weston C, Auperin A, Pinkerton R, Lambilliote A, et al. Excellent survival following two courses of COPAD chemotherapy in children and adolescents with resected localized B-cell non-Hodgkin’s lymphoma: results of the FAB/LMB 96 international study. Br J Haematol. 2008; 141:840–7.
Article15. Patte C, Philip T, Rodary C, Bernard A, Zucker JM, Bernard JL, et al. Improved survival rate in children with stage III and IV B cell non-Hodgkin’s lymphoma and leukemia using multi-agent chemotherapy: results of a study of 114 children from the French Pediatric Oncology Society. J Clin Oncol. 1986; 4:1219–26.
Article16. Gaynon PS, Steinherz PG, Bleyer WA, Ablin AR, Albo VC, Finklestein JZ, et al. Improved therapy for children with acute lymphoblastic leukemia and unfavorable presenting features: a follow-up report of the Childrens Cancer Group Study CCG-106. J Clin Oncol. 1993; 11:2234–42.
Article17. Meadows AT, Sposto R, Jenkin RD, Kersey JH, Chilcote RR, Siegel SE, et al. Similar efficacy of 6 and 18 months of therapy with four drugs (COMP) for localized non-Hodgkin’s lymphoma of children: a report from the Childrens Cancer Study Group. J Clin Oncol. 1989; 7:92–9.
Article18. Anderson JR, Jenkin RD, Wilson JF, Kjeldsberg CR, Sposto R, Chilcote RR, et al. Long-term follow-up of patients treated with COMP or LSA2L2 therapy for childhood non-Hodgkin’s lymphoma: a report of CCG-551 from the Childrens Cancer Group. J Clin Oncol. 1993; 11:1024–32.
Article19. Reiter A, Schrappe M, Ludwig WD, Tiemann M, Parwaresch R, Zimmermann M, et al. Intensive ALL-type therapy without local radiotherapy provides a 90% event-free survival for children with T-cell lymphoblastic lymphoma: a BFM group report. Blood. 2000; 95:416–21.20. Anoop P, Sankpal S, Stiller C, Tewari S, Lancaster DL, Khabra K, et al. Outcome of childhood relapsed or refractory mature B-cell non-Hodgkin lymphoma and acute lymphoblastic leukemia. Leuk Lymphoma. 2012; 53:1882–8.
Article21. Griffin TC, Weitzman S, Weinstein H, Chang M, Cairo M, Hutchison R, et al. A study of rituximab and ifosfamide, carboplatin, and etoposide chemotherapy in children with recurrent / refractory B-cell (CD20+) non-Hodgkin lymphoma and mature B-cell acute lymphoblastic leukemia: a report from the Children’s Oncology Group. Pediatr Blood Cancer. 2009; 52:177–81.22. Won SC, Han JW, Kwon SY, Shin HY, Ahn HS, Hwang TJ, et al. Autologous peripheral blood stem cell transplantation in children with non-Hodgkin’s lymphoma: a report from the Korean Society of Pediatric Hematology-Oncology. Ann Hematol. 2006; 85:787–94.
Article23. Lones MA, Sanger WG, Le Beau MM, Heerema NA, Sposto R, Perkins SL, et al. Chromosome abnormalities may correlate with prognosis in Burkitt/Burkitt-like lymphomas of children and adolescents: a report from Children’s Cancer Group Study CCG-E08. J Pediatr Hematol Oncol. 2004; 26:169–78.24. Knutsen T. Cytogenetic changes in the progression of lymphoma. Leuk Lymphoma. 1998; 31:1–19.
Article25. Poirel HA, Cairo MS, Heerema NA, Swansbury J, Auperin A, Launay E, et al. Specific cytogenetic abnormalities are associated with a significantly inferior outcome in children and adolescents with mature B-cell non-Hodgkin’s lymphoma: results of the FAB/LMB 96 international study. Leukemia. 2009; 23:323–31.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Optimal therapy for adolescents and young adults with acute lymphoblastic leukemia-current perspectives
- Treatment Outcome of Childhood B-cell Lymphoma and L3 Acute Lymphoblastic Leukemia from a Single Institution
- Treatment of Acute Lymphoblastic Leukemia in children
- Adolescents and young adults (AYA) with acute lymphoblastic leukemia
- Ifosfamide and Etoposide in Relapsed Refractory Childhood Acute Lymphoblastic Leukemia
