Treatment of Cerebral Vasospasm in an Infant Using a Modified Dotter Technique
- Affiliations
-
- 1Department of Neurological Surgery, University of Miami Miller School of Medicine, Miami, FL, USA. ericpete@med.miami.edu
- KMID: 2377626
- DOI: http://doi.org/10.7461/jcen.2017.19.1.48
Abstract
- An 8-month old female presented with spontaneous subarachnoid hemorrhage and was treated successfully with endovascular coil embolization of the ruptured aneurysm. Transcranial Doppler ultrasound performed four days later demonstrated middle cerebral artery (MCA) velocities greater than 350 cm/sec on the right and greater than 200 cm/sec on the left, despite medical management. The patient demonstrated no focal neurological deficits, though examination was limited by our patient's sedation and intubation. Angiography revealed severe vasospasm of the supraclinoid internal carotid and MCA territories, bilaterally. The vasospasm was refractory to the administration of intra-arterial verapamil. Balloon angioplasty was attempted, but the device could not be advanced safely due to the small size of the patient's vessels and the stiffness of the device. A microcatheter (0.0165" diameter) was advanced over a J-shaped soft microwire (0.014" diameter) to perform mechanical angioplasty in the internal carotid artery and MCA vessels bilaterally. Dramatic improvement was seen angiographically and on transcranial Doppler, and no complications were seen.
Keyword
MeSH Terms
Figure
-

Fig. 1 Angiography three days post aneurysm coiling revealed bilateral vasospasm of the supraclinoid ICA, ACA, and MCA territories. The vasospasm was greater than 60%, when compared to her initial angiogram. ICA = internal carotid artery; ACA = anterior cerebral artery; MCA = middle cerebral artery.
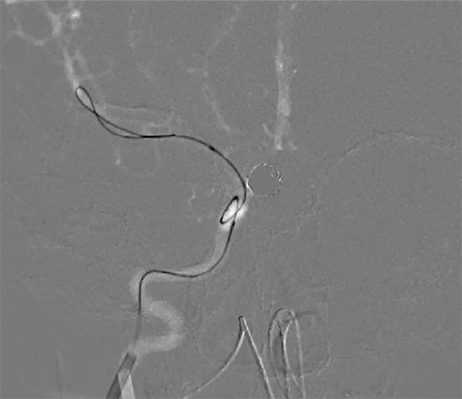
Fig. 2 The supraclinoid ICA and MCA were mechanically dilated bilaterally using a Marathon™ microcatheter (0.0165" diameter), which advanced over a J-shaped 0.014" soft Mirage™ microwire (0.014" diameter). ICA = internal carotid artery; MCA = middle cerebral artery.

Fig. 3 Post-procedural angiography revealed dramatic improvement as the proximal MCA M1 segment diameters increased to 1.0 in the right and 1.2 mm in the left. MCA = middle cerebral artery.
Reference
-
1. Aaslid R, Huber P, Nornes H. Evaluation of cerebrovascular spasm with transcranial Doppler ultrasound. J Neurosurg. 1984; 01. 60(1):37–41.
Article2. Dotter CT, Judkins MP. Percutaneous transluminal treatment of arteriosclerotic obstruction. Radiology. 1965; 04. 84:631–643.
Article3. Moftakhar P, Cooke DL, Fullerton HJ, Ko NU, Amans MR, Narvid JA, et al. Extent of collateralization predicting symptomatic cerebral vasospasm among pediatric patients: correlations among angiography, transcranial Doppler ultrasonography, and clinical findings. J Neurosurg Pediatr. 2015; 03. 15(3):282–290.
Article4. Ostergaard JR, Voldby B. Intracranial arterial aneurysms in children and adolescents. J Neurosurg. 1983; 06. 58(6):832–837.5. Proust F, Toussaint P, Garniéri J, Hannequin D, Legars D, Houtteville JP, et al. Pediatric cerebral aneurysms. J Neurosurg. 2001; 05. 94(5):733–739.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Prevention and Medical Management of Vasospasm
- Transcranial Doppler Monitoring in Subarachnoid Hemorrhage
- Middle Cerebral Artery Infarction Caused by Cerebral Vasospasm After Brain Tumor Surgery by Pterional Approach
- Relation between Thromboembolism and Delayed Ischemic Neurological Deficits in Aneurysmal Subarachnoid Hemorrhage
- Cerebral Vasospasm After Traumatic Subarachnoid Hemorrhage and Its Risk Factor: Combined Periodic Follow Up of Transcranial Doppler and CT Angiography
