Quadricuspid Aortic Valve Complicated with Severe Aortic Regurgitation and Left-Sided Inferior Vena Cava
- Affiliations
-
- 1Department of Cardiology, Kyoto First Red Cross Hospital, Kyoto, Japan. risa11221998@yahoo.co.jp
- 2Department of Cardiovascular Surgery, Kyoto First Red Cross Hospital, Kyoto, Japan.
- 3Department of Emergency Medicine, Kyoto First Red Cross Hospital, Kyoto, Japan.
- KMID: 2375295
- DOI: http://doi.org/10.4250/jcu.2017.25.1.34
Abstract
- No abstract available.
MeSH Terms
Figure
-
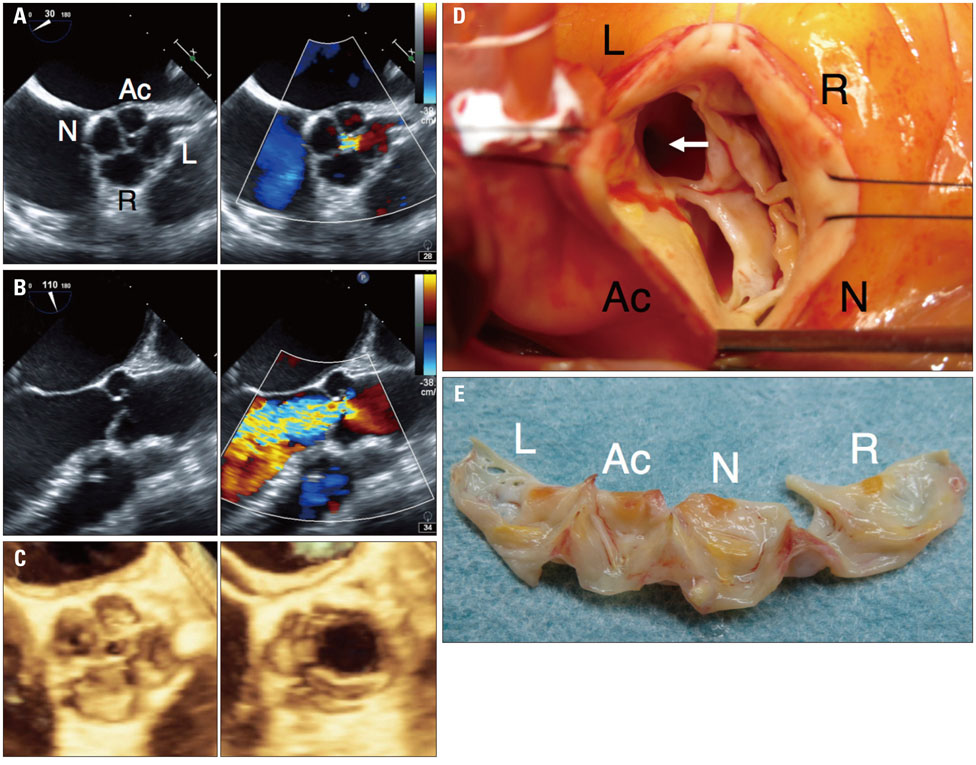
Fig. 1 Quadricuspid aortic valve with severe aortic regurgitation. A and B: Two-dimensional transesophageal echocardiography images during diastolic phase (A, short-axis view; B, long-axis view). C: Three-dimensional transesophageal echocardiography images (left, diastolic; right, systolic). D: Intraoperative photograph showing quadricuspid aortic valve and left main ostium (white arrow). The accessory cusp was located between the left coronary cusp and the non-coronary cusp. E: Surgically resected leaflets of the quadricuspid aortic valve showing 1 larger cusp (R), 2 intermediate cusps (L and N), and 1 smaller cusp (Ac), corresponding to type D based on the Hurwitz and Roberts' classification. Ac: accessory cusp, L: left coronary cusp, N: non-coronary cusp, R: right coronary cusp.
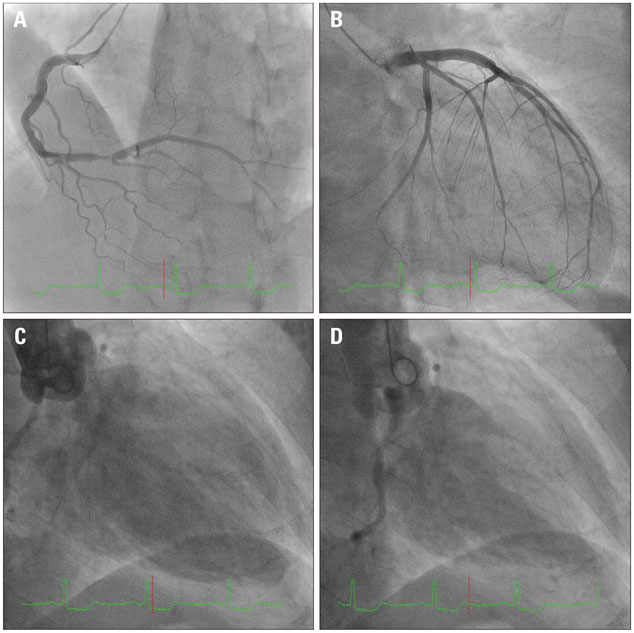
Fig. 2 Pre-operative cardiac catheterization. Coronary angiography (CAG) (A, right CAG; B, left CAG) and aortography (C, end-diastolic; D, end-systolic) depicted a significant stenosis in the distal segment of right coronary artery and aortic regurgitation of Sellers grade 3, respectively.
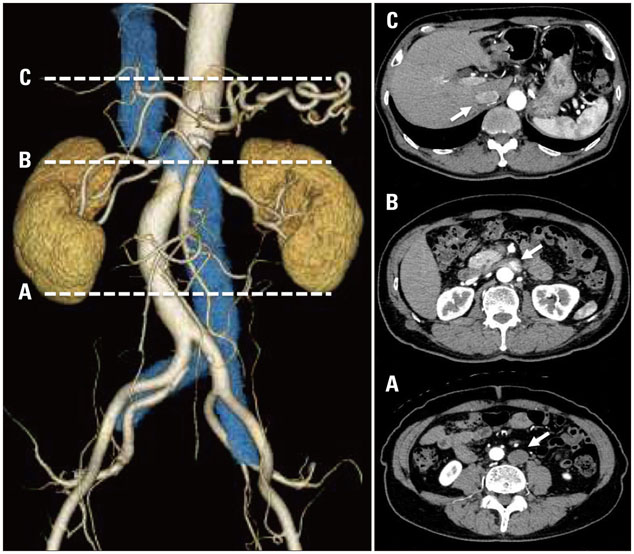
Fig. 3 Pre-operative computed tomography images indicating the left-sided inferior vena cava (IVC) (left: reconstructed 3-dimensional image, right: transverse image). The IVC (white arrows) ran upward along the left side of the aorta (A), crossed the aorta anteriorly through the meso-aortic angle (B), and communicated with a normally positioned infra-hepatic IVC (C).
Reference
-
1. Feldman BJ, Khandheria BK, Warnes CA, Seward JB, Taylor CL, Tajik AJ. Incidence, description and functional assessment of isolated quadricuspid aortic valves. Am J Cardiol. 1990; 65:937–938.2. Tsang MY, Abudiab MM, Ammash NM, Naqvi TZ, Edwards WD, Nkomo VT, Pellikka PA. Quadricuspid aortic valve: characteristics, associated structural cardiovascular abnormalities, and clinical outcomes. Circulation. 2016; 133:312–319.3. D'Aloia A, Vizzardi E, Bugatti S, Chiari E, Repossini A, Muneretto C, Dei Cas L. A quadricuspid aortic valve associated with severe aortic regurgitation and left ventricular systolic dysfunction. Eur J Echocardiogr. 2009; 10:724–725.4. Brugts JJ, Cuypers JA, Polak P, Ouhlous M, van de Woestijne P, Wessels M, Roos-Hesselink J. Quadricuspid aortic valve and anomalous systemic venous connection in a patient with cat-eye syndrome. Circulation. 2015; 131:1225–1227.5. Ang WC, Doyle T, Stringer MD. Left-sided and duplicate inferior vena cava: a case series and review. Clin Anat. 2013; 26:990–1001.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Left-Sided Inferior Vena Cava Associated with Abdominal Aortic Aneurysm
- Quadricuspid Aortic Valve : Report of Three Cases and Review of the Literature
- A Case of 51 Year Old Woman with Quadricuspid Aortic Valve Associated with Regurgitation
- Congenital Quadricuspid Aortic Valve
- Congenital Quadricuspid Aortic Valve Disease
