J Korean Neurosurg Soc.
2017 Feb;60(2):220-224. 10.3340/jkns.2016.1010.015.
Lumbar Disc Herniation Presented with Contralateral Symptoms
- Affiliations
-
- 1Department of Neurosurgery, College of Medicine, Chosun University, Gwangju, Korea. chosunns@chosun.ac.kr
- 2Department of Neurosurgery, Suwon Nanoori Hospital, Suwon, Korea.
- KMID: 2374884
- DOI: http://doi.org/10.3340/jkns.2016.1010.015
Abstract
OBJECTIVE
This study aimed to unravel the putative mechanism underlying the neurologic deficits contralateral to the side with lumbar disc herniation (LDH) and to elucidate the treatment for this condition.
METHODS
From January 2009 to June 2015, 8 patients with LDH with predominantly contralateral neurologic deficits underwent surgical treatment on the side with LDH with or without decompressing the symptomatic side. A retrospective review of charts and radiological records of these 8 patients was performed. The putative mechanisms underlying the associated contralateral neurological deficits, magnetic resonance imaging (MRI), electromyography (EMG), and the adequate surgical approach are discussed here.
RESULTS
MRI revealed a similar laterally skewed paramedian disc herniation, with the apex deviated from the symptomatic side rather than directly compressing the nerve root; this condition may generate a contralateral traction force. EMG revealed radiculopathies in both sides of 6 patients and in the herniated side of 2 patients. Based on EMG findings and the existence of suspicious lateral recess stenosis of the symptomatic side, 6 patients underwent bilateral decompression of nerve roots and 2 were subjected to a microscopic discectomy to treat the asymptomatic disc herniation. No specific conditions such as venous congestion, nerve root anomaly or epidural lipomatosis were observed, which may be considered the putative pathomechanism causing the contralateral neurological deficits. The symptoms resolved significantly after surgery.
CONCLUSION
The traction force generated on the contralateral side and lateral recess stenosis, rather than direct compression, may cause the contralateral neurologic deficits observed in LDH.
Keyword
MeSH Terms
Figure
-

Fig. 1 A 67-year-old male patient presented with right leg motor weakness. A and B: T2-weighted sagittal and axial magnetic resonance images show left paracentral disc herniation with the apex deviated to the left.
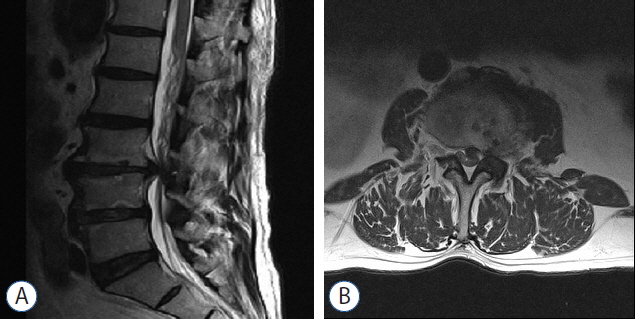
Fig. 2 A 50-year-old male patient presented with right leg pain. A and B: T2-weighted sagittal and axial magnetic resonance images reveal left paracentral disc herniation with the apex deviated to the left. Neither of the nerve roots are directly compressed.
Reference
-
References
1. Auld AW, DeWall JG. Myelographic defect on the side opposite the leg pain. A case report with an explanation of mechanism of action. Spine (Phila Pa 1976). 4:174–175. 1979.2. Chou H, Tsutsumi T, Saito M, Kogame M, Kim T, Asai T. Ll/2 disc herniation with flaccid paralysis of contralateral lower cxtremity-a case report. Rinsho Seikei Geka. 21:107–111. 1986.3. Choudhury AR, Taylor JC, Worthington BS, Whitaker R. Lumbar radiculopathy contralateral to upper lumbar disc herniation: report of 3 cases. Br J Surg. 65:842–844. 1978.
Article4. Hayashi M, Yoshida A. First and second lumbar disc herniation with symptoms of the contralateral extremity; a case report. Seikeigeka. 54:1402–1405. 2003.5. Hasegawa T, Imai Y, Katsuno R, Ohnaru K, Saeki T, Mikawa Y. Lumbar radiculopathy contralateral to the side of lumbar disc herniation. Kawasaki Med J. 31:47–54. 2005.6. Higashi T, Tanimoto M, Honda A, Numazaki S, Tatara Y, Kobayashi A. Single 1umbar disc herniation with contralateral two nerve roots involvement: a case report. Seikeigeka. 53:57–59. 2002.7. Jensen MC, Brant-Zawadzki MN, Obuchowski N, Modic MT, Malkasian D, Ross JS. Magnetic resonance imaging of the lumbar spine in people without back pain. N Engl J Med. 331:69–73. 1994.
Article8. Kalemci O, Kizmazoglu C, Ozer E, Arda MN. Lumbar disc herniation associated with contralateral neurological deficit: can venous congestion be the cause? Asian Spine J. 7:60–2. 2013.
Article9. Kornberg M. Sciatica contralateral to lumbar disk herniation. Orthopedics. 17:362–364. 1994.
Article10. Mirovsky Y, Halperin N. Eccentric compression of the spinal canal causing dominantly contralateral-side symptoms. J Spinal Disord. 13:174–177. 2000.
Article11. Miyashita H, Kumano K, Yokozeki H. Sciatica on the opposite side of lumbar disc herniation a case report. Bessatsu Seikei Geka. 13:81–82. 1998.12. Shimamura T, Ohsawa Y, Yamaki K, Kaiyama j, Abe M. A case report of lumbar disc herniation with contralateral symptoms. Seikeigeka. 42:1233–1236. 1991.13. Sucu HK, Gelal F. Lumbar disc herniation with contralateral symptoms. Eur Spine J. 15:570–574. 2006.14. Weishaupt D, Zanetti M, Hodler J, Boos N. MR imaging of the lumbar spine: prevalence of intervertebral disk extrusion and sequestration, nerve root compression, end plate abnormalities, and osteoarthritis of the facet joints in asymptomatic volunteers. Radiology. 209:661–666. 1998.
Article15. Wilberger JE Jr, Pang D. Syndrome of the incidental herniated lumbar disc. J Neurosurg. 59:137–141. 1983.
Article16. Yang JS, Zhang DJ, Hao DJ. Lumbar disc herniation with contralateral radiculopathy: do we neglect the epidural fat? Pain Physician. 18:253–256. 2015.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Lumbar Disc Herniation Associated with Contralateral Neurological Deficit: Can Venous Congestion Be the Cause?
- Rapid Repeated Recurrent Lumbar Disc Herniation after Microscopic Discectomies
- Juvenile Lumbar Intervertebral Disc Herniation: Five Cases Report
- Clinical Analysis of Recurrent Lumbar Disc Herniation
- Ordinary Disc Herniation Changing into Posterior Epidural Migration of Lumbar Disc Fragments Confirmed by Magnetic Resonance Imaging: A Case Report of a Successful Endoscopic Treatment
