Spontaneous dissections of multiple visceral arteries: an extremely rare case
- Affiliations
-
- 1Endovascular Training Center, Inha University Hospital, Incheon, Korea.
- 2Department of Radiology, Inha University School of Medicine, Incheon, Korea. radjeon@inha.ac.kr
- 3Department of Vascular Surgery, Inha University School of Medicine, Incheon, Korea.
- KMID: 2374689
- DOI: http://doi.org/10.4174/astr.2017.92.4.225
Abstract
- Spontaneous dissections of visceral arteries without aortic involvement are very rare. The etiologies of these entities are unclear and their clinical managements remain controversial. We report a case of spontaneous multiple dissections affecting 4 visceral arteries including the superior mesenteric artery, the celiac artery and the bilateral renal arteries. The patient was managed conservatively and endovascularly. The clinical manifestation markedly improved and laboratory tests returned to normal limits within 1 week. The regular follow-up suggested a good clinical and radiological outcome until 84 months.
MeSH Terms
Figure
-
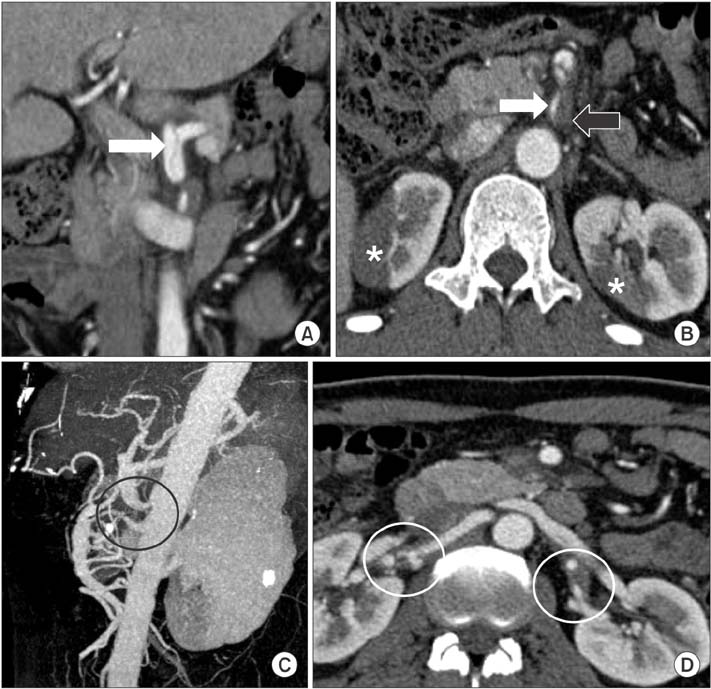
Fig. 1 Emergency computed tomographic angiography was obtained on admission. (A) Coronal reconstruction image demonstrated a dissection of the celiac trunk spreading from ostium to the proximal splenic artery with intimal flap (white arrow). The true lumen provides perfusion to the splenic artery while hepatic artery was perfused from the false lumen (not shown). (B–D) An approximately 4-cm-long dissection of the superior mesenteric artery from orifice with thrombus formation in the false lumen (black arrow) and severely narrow true lumen (white arrow) were evident on axial and maximum intensity projection sagittal reconstruction image (black circle). Bilateral focal renal infarctions (asterisk) were also noticed as a consequence of corresponding renal artery dissections (white circle).
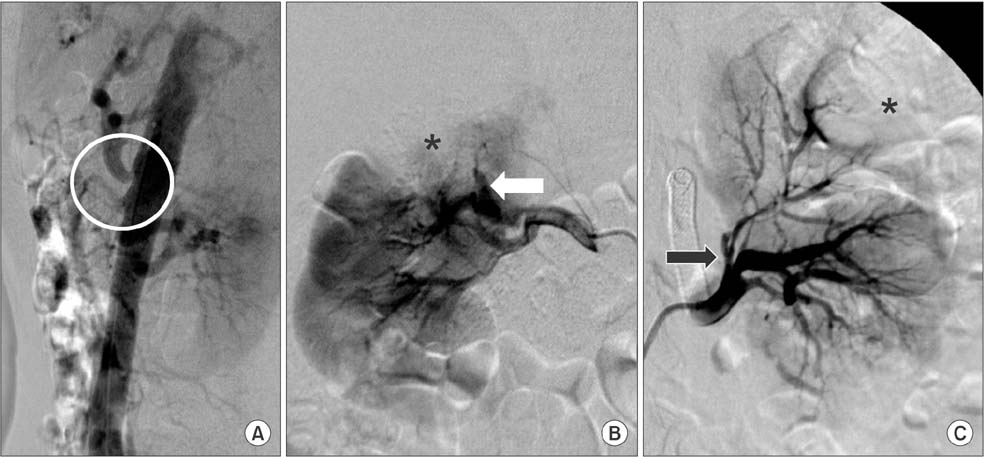
Fig. 2 Aortogram and selective bilateral renal arteriograms confirmed multiple arterial dissections. (A) Proximal dissections of the celiac artery and superior mesenteric artery (circle) were demonstrated on the lateral aortogram. A guide wire was able to pass through the narrowing segment; 2 balloon-expandable stents were then deployed. Poststenting angiogram showed remarkable dilation of the true lumen (not shown). (B) Dissection of the superior segmental artery (white arrow) and subsequent upper pole infarction (asterisk) was seen on the right renal arteriogram. (C) Left renal arteriogram revealed the dissection and narrowing at the bifurcation level of the anterior division and the superior segmental artery (black arrow) with the corresponding perfusion defect in the upper pole (asterisk). A guiding catheter was exchanged, followed by the deployment of a 6-mm × 2-cm balloon-expandable renal stent at the level of bifurcation to the anterior division. Complete angiogram demonstrated full dilatation of the previous narrowing segment (not shown).

Fig. 3 Follow-up computed tomographic angiography obtained 54 months after treatment. (A) The false lumen of the celiac artery dissection remained patent and unchanged in size, constituting a stable and chronic dissection without flow disturbance. (B–D) The superior mesenteric artery and left renal stents were patent. Reperfusion was evident in the right renal upper pole whereas left renal upper pole was calcified and atrophied (circle).
Cited by 1 articles
-
Antithrombotic therapy has no beneficial effect in conservative treatment of spontaneous isolated superior mesenteric arterial dissection
Young Sup Yoo, Soo Jin Na Choi, Ho Kyun Lee
Ann Surg Treat Res. 2021;100(3):166-174. doi: 10.4174/astr.2021.100.3.166.
Reference
-
1. Zeina AR, Nachtigal A, Mahamid A, Soimu U, Ashkenazi I, Oster M. Isolated spontaneous dissection of a visceral artery: a rare cause of epigastric pain. Emerg Radiol. 2015; 22:215–220.2. Jung SC, Lee W, Park EA, Jae HJ, Chung JW, Park JH. Spontaneous dissection of the splanchnic arteries: CT findings, treatment, and outcome. AJR Am J Roentgenol. 2013; 200:219–225.3. Katz-Summercorn AC, Borg CM, Harris PL. Spontaneous renal artery dissection complicated by renal infarction: a case report and review of the literature. Int J Surg Case Rep. 2012; 3:257–259.4. Jain A, Tracci MC, Coleman DM, Cherry KJ, Upchurch GR Jr. Renal malperfusion: spontaneous renal artery dissection and with aortic dissection. Semin Vasc Surg. 2013; 26:178–188.5. Takayama T, Miyata T, Shirakawa M, Nagawa H. Isolated spontaneous dissection of the splanchnic arteries. J Vasc Surg. 2008; 48:329–333.6. Takach TJ, Madjarov JM, Holleman JH, Robicsek F, Roush TS. Spontaneous splanchnic dissection: application and timing of therapeutic options. J Vasc Surg. 2009; 50:557–563.7. Bonardelli S, Battaglia G, Zanotti C, Cervi E, Guadrini C, Giulini SM. Sequential multiple visceral arteries dissections without aortic involvement. Ann Vasc Surg. 2013; 27:497.e9–497.e13.8. Gobble RM, Brill ER, Rockman CB, Hecht EM, Lamparello PJ, Jacobowitz GR, et al. Endovascular treatment of spontaneous dissections of the superior mesenteric artery. J Vasc Surg. 2009; 50:1326–1332.9. DiMusto PD, Oberdoerster MM, Criado E. Isolated celiac artery dissection. J Vasc Surg. 2015; 61:972–976.10. Takayama Y, Takao M, Inoue T, Yoshimi F, Koyama K, Nagai H. Isolated spontaneous dissection of the celiac artery: report of two cases. Ann Vasc Dis. 2014; 7:64–67.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Ischemic Infarctions in Young Men Secondary to Traumatic and Spontaneous Intracranial Arteries Dissection
- Spontaneous Isolated Dissection of the Celiac Artery: a Case Report
- Spontaneous Visceral Artery Hemorrhage in a Patient with Systemic Lupus Erythematosus Combined with Antiphospholipid Syndrome: A Case Report
- A Case of Vascular Ehlers-Danlos Syndrome Presenting with Multiple Cerebral Arterial Dissections
- A Case of Spontaneous Renal Artery and Celiac Artery Dissection in Healthy Man
