Acetic acid sclerotherapy for treatment of biliary leak from an isolated right posterior sectoral duct after cholecystectomy
- Affiliations
-
- 1Department of Surgery, Inje University Haeundae Paik Hospital, Inje University College of Medicine, Busan, Korea. jipark@paik.ac.kr
- 2Department of Surgery, Inje University Busan Paik Hospital, Inje University College of Medicine, Busan, Korea.
- KMID: 2374688
- DOI: http://doi.org/10.4174/astr.2017.92.4.221
Abstract
- Bile duct injury is one of the most serious complications of both laparoscopic and open cholecystectomy. Isolated bile duct injury can occur from the misidentification of aberrant right hepatic ducts, and it is troublesome because the early diagnosis is easy to miss and the definite treatment is controversial. We report a case of an isolated right posterior sectoral duct injury following cholecystectomy managed successfully with acetic acid sclerotherapy combined with coil embolization for a fistula tract.
Keyword
MeSH Terms
Figure
-
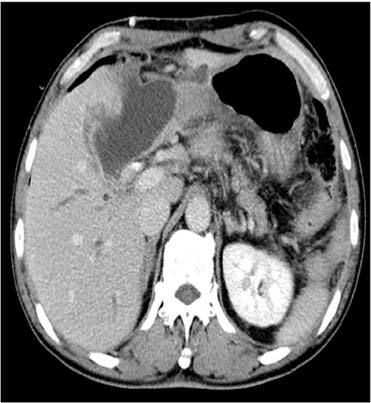
Fig. 1 Abdomen CT scan showed complicated fluid collection in gallbladder bed.
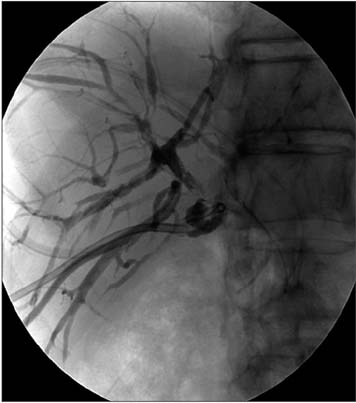
Fig. 2 Percutaneous transhepatic biliary drainage cholangiogram revealed biliary leak from the right posterior sectoral duct.
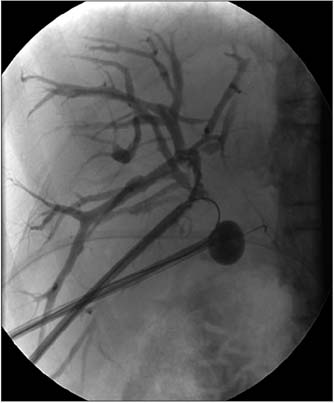
Fig. 3 The injection of 50% acetic acid into the isolated right posterior sectoral duct was performed via a percutaneous transhepatic biliary drainage tract and was maintained for 10 minutes. The 7-F balloon occlusion catheter (Boston Scientific, Watertown, MA, USA) was used simultaneously to prevent leakage of the injected acetic acid into the fistula tract.

Fig. 4 Coil embolization was performed for the fistula tract between the right posterior sectoral duct and abscess cavity because of sustained biliary leakage after three sessions of acetic acid sclerotherapy.

Fig. 5 Abdomen CT scan taken 20 days after acetic acid sclerotherapy shows disappearance of subhepatic biloma.
Reference
-
1. Perini RF, Uflacker R, Cunningham JT, Selby JB, Adams D. Isolated right segmental hepatic duct injury following laparoscopic cholecystectomy. Cardiovasc Intervent Radiol. 2005; 28:185–195.2. Hwang S, Lee SG, Lee YJ, Ha TY, Ko GY, Song GW. Delayed-onset isolated injury of the right posterior segment duct after laparoscopic cholecystectomy: a report of hepatic segmental atrophy induction. Surg Laparosc Endosc Percutan Tech. 2007; 17:203–205.3. Colovic RB. Isolated segmental, sectoral and right hepatic bile duct injuries. World J Gastroenterol. 2009; 15:1415–1419.4. Mazer LM, Tapper EB, Sarmiento JM. Nonoperative management of right posterior sectoral duct injury following laparoscopic cholecystectomy. J Gastrointest Surg. 2011; 15:1237–1242.5. Wojcicki M, Patkowski W, Chmurowicz T, Bialek A, Wiechowska-Kozlowska A, Stankiewicz R, et al. Isolated right posterior bile duct injury following cholecystectomy: report of two cases. World J Gastroenterol. 2013; 19:6118–6121.6. Choi G, Eun CK, Choi H. Acetic acid sclerotherapy for treatment of a bile leak from an isolated bile duct after laparoscopic cholecystectomy. Cardiovasc Intervent Radiol. 2011; 34:Suppl 2. S303–S306.7. Park JH, Oh JH, Yoon Y, Hong SH, Park SJ. Acetic acid sclerotherapy for treatment of a biliary leak from an isolated bile duct after hepatic surgery. J Vasc Interv Radiol. 2005; 16:885–888.8. Matsumoto T, Iwaki K, Hagino Y, Kawano K, Kitano S, Tomonari K, et al. Ethanol injection therapy of an isolated bile duct associated with a biliary-cutaneous fistula. J Gastroenterol Hepatol. 2002; 17:807–810.9. Kyokane T, Nagino M, Sano T, Nimura Y. Ethanol ablation for segmental bile duct leakage after hepatobiliary resection. Surgery. 2002; 131:111–113.10. Ohnishi K, Ohyama N, Ito S, Fujiwara K. Small hepatocellular carcinoma: treatment with US-guided intratumoral injection of acetic acid. Radiology. 1994; 193:747–752.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Successful non-surgical treatment for isolated right anterior section bile duct injury following laparoscopic cholecystectomy: Report of a case
- Therapeutic induction of hepatic atrophy for isolated injury of the right posterior sectoral duct following laparoscopic cholecystectomy
- Isolated aberrant right cysticohepatic duct injury during laparoscopic cholecystectomy: Evaluation and treatment challenges of a severe postoperative complication associated with an extremely rare anatomical variant
- Minimal invasive treatment of biliary leak after laparoscopic cholecystectomy
- A Case of Bile Leak from the Accessory Bile Duct after Laparoscopic Cholecystectomy
