Bilateral Scapulohumeral Ankylosis after Prolonged Mechanical Ventilation
- Affiliations
-
- 1Division of Orthopaedic Surgery, Spaarne Gasthuis, Spaarnepoort, Hoofddorp, Netherlands. mlvanlotten@gmail.com
- 2Division of Anaesthesiology, VU University Medical Centre, De Boelelaan, Amsterdam, Netherlands.
- KMID: 2374283
- DOI: http://doi.org/10.4055/cios.2016.8.3.339
Abstract
- This case demonstrates a rarely reported bilateral scapulohumeral bony ankylosis. A young woman developed extensive heterotopic ossifications (HOs) in both shoulder joints after being mechanically ventilated for several months at the intensive care unit in a comatose status. She presented with a severe movement restriction of both shoulder joints. Surgical resection of the bony bridges was performed in 2 separate sessions with a significant improvement of shoulder function afterwards. No postoperative complications, pain, or recurrence of HOs were noted at 1-year follow-up. Mechanical ventilation, immobilization, neuromuscular blockage, and prolonged sedation are known risk factors for the development of HOs in the shoulder joints. Relatively early surgical resection of the HOs can be performed safely in contrary to earlier belief. Afterwards, nonsteroidal anti-inflammatory drugs and/or radiation therapy can be possible treatment modalities to prevent recurrence of HOs.
MeSH Terms
Figure
-
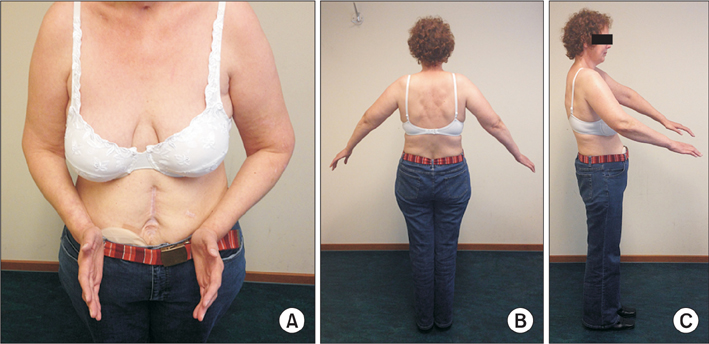
Fig. 1 Preoperative range of motion of the arms. (A) Neutral position. (B) Maximal abduction. (C) Maximal anteflexion.

Fig. 2 Preoperative roentgenogram of the right shoulder joint (A) and the left shoulder joint (B).
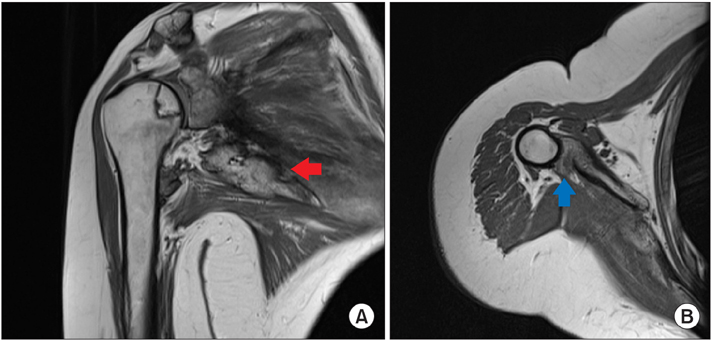
Fig. 3 Magnetic resonance imaging showing avascular necrosis of the humeral head and isolated ossifications in the subscapularis muscle (red arrow) in the coronal plane (A) and a complete bony bridge located in the teres minor muscle (blue arrow) in the transverse plane (B).

Fig. 4 Three-dimensional computed tomography reconstruction image showing isolated ossifications in the subscapularis muscle (red arrow) and the complete bony bridge in the teres minor muscle (blue arrow).
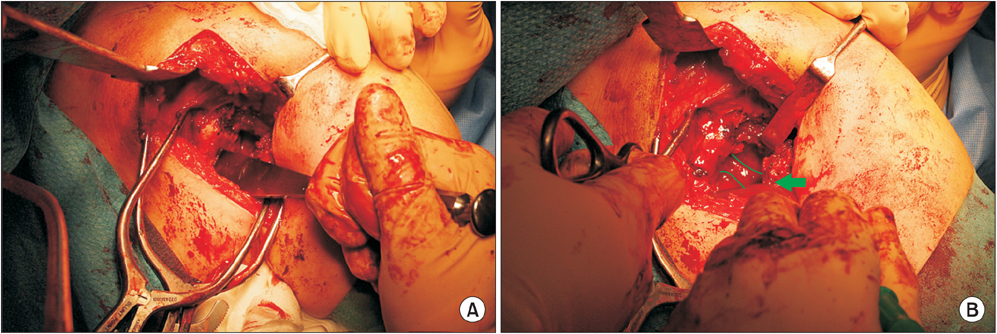
Fig. 5 (A) Resection of the bony bridge via posterior approach with an osteotome. (B) Identification of the radial nerve in close proximity to the bony bridge (arrow).

Fig. 6 Postoperative shoulder function in the sagittal plane (A) and in the coronal plane (B), maximal exorotation.

Fig. 7 One-year postoperative roentgenogram of the right shoulder (A) and the left shoulder (B) without recurrence of heterotopic ossifications.
Reference
-
1. Tsionos I, Leclercq C, Rochet JM. Heterotopic ossification of the elbow in patients with burns: results after early excision. J Bone Joint Surg Br. 2004; 86(3):396–403.2. Nauth A, Giles E, Potter BK, et al. Heterotopic ossification in orthopaedic trauma. J Orthop Trauma. 2012; 26(12):684–688.
Article3. Christakou A, Alimatiri M, Kouvarakos A, et al. Heterotopic ossification in critical ill patients: a review. Int J Physiother Res. 2013; 1(4):188–195.4. Chalmers J, Gray DH, Rush J. Observations on the induction of bone in soft tissues. J Bone Joint Surg Br. 1975; 57(1):36–45.
Article5. Pansard E, Schnitzler A, Lautridou C, Judet T, Denormandie P, Genet F. Heterotopic ossification of the shoulder after central nervous system lesion: indications for surgery and results. J Shoulder Elbow Surg. 2013; 22(6):767–774.
Article6. An HS, Ebraheim N, Kim K, Jackson WT, Kane JT. Heterotopic ossification and pseudoarthrosis in the shoulder following encephalitis: a case report and review of the literature. Clin Orthop Relat Res. 1987; (219):291–298.7. Kir MC, Ozdemir MT. Myositis ossificans around shoulder following military training programme. Indian J Orthop. 2011; 45(6):573–575.
Article8. Garland DE. A clinical perspective on common forms of acquired heterotopic ossification. Clin Orthop Relat Res. 1991; (263):13–29.
Article9. Zeckey C, Hildebrand F, Frink M, Krettek C. Heterotopic ossifications following implant surgery: epidemiology, therapeutical approaches and current concepts. Semin Immunopathol. 2011; 33(3):273–286.
Article10. Sell S, Willms R, Jany R, et al. The suppression of heterotopic ossifications: radiation versus NSAID therapy: a prospective study. J Arthroplasty. 1998; 13(8):854–859.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Comparative Study of Central Venous Pressure Measurements during Mechanical Ventilation and after Disconnection of Ventilation
- Treatment of acute respiratory failure: invasive mechanical ventilation
- Respiratory Failure in Guillain-Barre Syndrome
- Observation of Treatment Outcome with Radiography in Adhesive Capsulitis of Shoulder
- Mechanical Ventilation of the Children
