Coronary Computed Tomographic Angiography Does Not Accurately Predict the Need of Coronary Revascularization in Patients with Stable Angina
- Affiliations
-
- 1Department of Internal Medicine, Sanggye Paik Hospital, Inje University College of Medicine, Seoul, Korea.
- 2Department of Internal Medicine, School of Medicine, Kangwon National University, Chuncheon, Korea.
- 3Department of Internal Medicine, Myongji Hospital, Goyang, Korea.
- 4Department of Internal Medicine, Chung-Ang University Medical Center, Seoul, Korea.
- 5Department of Internal Medicine, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
- 6Department of Internal Medicine, Gil Hospital, Gachon University College of Medicine, Incheon, Korea.
- 7Department of Internal Medicine, Severance Cardiovascular Hospital, Yonsei University Health System, Seoul, Korea. mkhong61@yuhs.ac
- 8Cardiovascular Research Institute, Yonsei University College of Medicine, Seoul, Korea.
- 9Severance Biomedical Science Institute, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 2374151
- DOI: http://doi.org/10.3349/ymj.2016.57.5.1079
Abstract
- PURPOSE
To evaluate the ability of coronary computed tomographic angiography (CCTA) to predict the need of coronary revascularization in symptomatic patients with stable angina who were referred to a cardiac catheterization laboratory for coronary revascularization.
MATERIALS AND METHODS
Pre-angiography CCTA findings were analyzed in 1846 consecutive symptomatic patients with stable angina, who were referred to a cardiac catheterization laboratory at six hospitals and were potential candidates for coronary revascularization between July 2011 and December 2013. The number of patients requiring revascularization was determined based on the severity of coronary stenosis as assessed by CCTA. This was compared to the actual number of revascularization procedures performed in the cardiac catheterization laboratory.
RESULTS
Based on CCTA findings, coronary revascularization was indicated in 877 (48%) and not indicated in 969 (52%) patients. Of the 877 patients indicated for revascularization by CCTA, only 600 (68%) underwent the procedure, whereas 285 (29%) of the 969 patients not indicated for revascularization, as assessed by CCTA, underwent the procedure. When the coronary arteries were divided into 15 segments using the American Heart Association coronary tree model, the sensitivity, specificity, positive predictive value, and negative predictive value of CCTA for therapeutic decision making on a per-segment analysis were 42%, 96%, 40%, and 96%, respectively.
CONCLUSION
CCTA-based assessment of coronary stenosis severity does not sufficiently differentiate between coronary segments requiring revascularization versus those not requiring revascularization. Conventional coronary angiography should be considered to determine the need of revascularization in symptomatic patients with stable angina.
MeSH Terms
Figure
-

Fig. 1 Study flow diagram. The actual revascularization was performed in 600 (68%) of the 877 patients indicated for revascularization and in 285 (29%) of the 969 patients not indicated for revascularization. CCTA, coronary computed tomographic angiography.
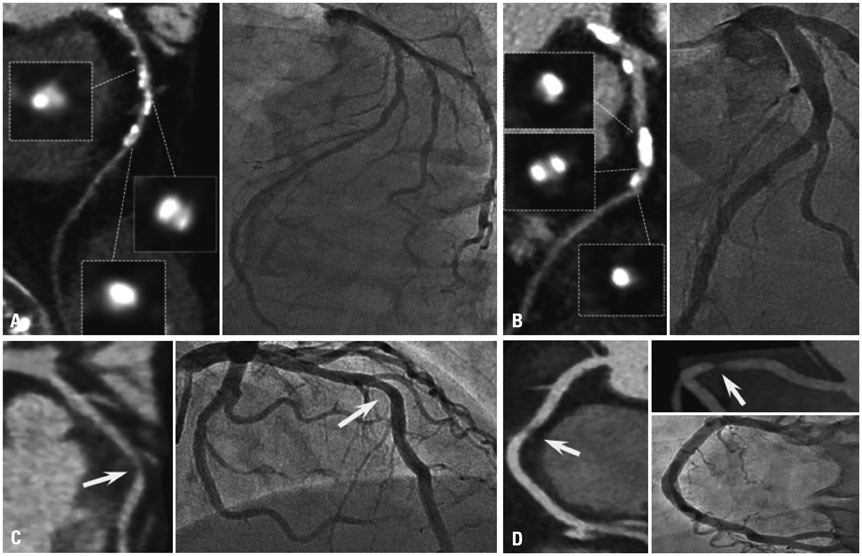
Fig. 2 Representative false positive cases for needing revascularization based on the coronary computed tomographic angiography (CCTA). (A) CCTA falsely identified this patient as a candidate for revascularization, based on the diffuse calcification of left anterior descending artery (LAD). (B) A second false-positive was indicated for revascularization because of a heavily calcified lesion within the LAD. (C) LAD was falsely identified as requiring revascularization because of lesion severity overestimation (arrow). (D) This right coronary artery was falsely indicated for revascularization because of a motion artifact (arrow). Right images of each panel (A, B, and C) are CCTA and left images are conventional coronary angiography. In panel (D), right and left upper images are CCTA and left lower image is conventional coronary angiography.

Fig. 3 Example of discordance between the coronary computed tomographic angiography (CCTA)-indicated therapy and the actual conducted therapy. Panel (A) and (B) are the CCTA and conventional coronary angiography images, respectively, from the same patient. (A) This patient was originally referred for need of revascularization of the left anterior descending artery based on the CCTA images (white arrow); however, revascularization was not performed (black arrow). Right image is CCTA and left image is conventional coronary angiography. (B) The same patient actually underwent revascularization of the left circumflex artery, which was not originally indicated based on CCTA images (white arrow); however, revascularization was performed (black arrow with solid line, before revascularization; black arrow with dotted line, after revascularization). Right image is CCTA, and middle and left images are conventional coronary angiography (before and after percutaneous coronary intervention, respectively).
Cited by 1 articles
-
Clinical Implications of Moderate Coronary Stenosis on Coronary Computed Tomography Angiography in Patients with Stable Angina
Choongki Kim, Sung-Jin Hong, Chul-Min Ahn, Jung-Sun Kim, Byeong-Keuk Kim, Young-Guk Ko, Byoung-Wook Choi, Donghoon Choi, Yangsoo Jang, Myeong-Ki Hong
Yonsei Med J. 2018;59(8):937-944. doi: 10.3349/ymj.2018.59.8.937.
Reference
-
1. Miller JM, Rochitte CE, Dewey M, Arbab-Zadeh A, Niinuma H, Gottlieb I, et al. Diagnostic performance of coronary angiography by 64-row CT. N Engl J Med. 2008; 359:2324–2336.
Article2. Meijboom WB, Meijs MF, Schuijf JD, Cramer MJ, Mollet NR, van Mieghem CA, et al. Diagnostic accuracy of 64-slice computed tomography coronary angiography: a prospective, multicenter, multivendor study. J Am Coll Cardiol. 2008; 52:2135–2144.
Article3. Schuetz GM, Zacharopoulou NM, Schlattmann P, Dewey M. Meta-analysis: noninvasive coronary angiography using computed tomography versus magnetic resonance imaging. Ann Intern Med. 2010; 152:167–177.
Article4. Taylor AJ, Cerqueira M, Hodgson JM, Mark D, Min J, O'Gara P, et al. ACCF/SCCT/ACR/AHA/ASE/ASNC/NASCI/SCAI/SCMR 2010 Appropriate Use Criteria for Cardiac Computed Tomography. A Report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, the Society of Cardiovascular Computed Tomography, the American College of Radiology, the American Heart Association, the American Society of Echocardiography, the American Society of Nuclear Cardiology, the North American Society for Cardiovascular Imaging, the Society for Cardiovascular Angiography and Interventions, and the Society for Cardiovascular Magnetic Resonance. Circulation. 2010; 122:e525–e555.5. Min JK, Berman DS, Dunning A, Achenbach S, Al-Mallah M, Budoff MJ, et al. All-cause mortality benefit of coronary revascularization vs. medical therapy in patients without known coronary artery disease undergoing coronary computed tomographic angiography: results from CONFIRM (COronary CT Angiography EvaluatioN For Clinical Outcomes: an InteRnational Multicenter Registry). Eur Heart J. 2012; 33:3088–3097.
Article6. de Feyter PJ, Nieman K. CCTA to guide revascularization for high-risk CAD: a 'cliff hanger'. Eur Heart J. 2012; 33:3011–3013.
Article7. Shaw LJ, Hausleiter J, Achenbach S, Al-Mallah M, Berman DS, Budoff MJ, et al. Coronary computed tomographic angiography as a gatekeeper to invasive diagnostic and surgical procedures: results from the multicenter CONFIRM (Coronary CT Angiography Evaluation for Clinical Outcomes: an International Multicenter) registry. J Am Coll Cardiol. 2012; 60:2103–2114.8. Piers LH, Dikkers R, Willems TP, de Smet BJ, Oudkerk M, Zijlstra F, et al. Computed tomographic angiography or conventional coronary angiography in therapeutic decision-making. Eur Heart J. 2008; 29:2902–2907.
Article9. Moscariello A, Vliegenthart R, Schoepf UJ, Nance JW Jr, Zwerner PL, Meyer M, et al. Coronary CT angiography versus conventional cardiac angiography for therapeutic decision making in patients with high likelihood of coronary artery disease. Radiology. 2012; 265:385–392.
Article10. Austen WG, Edwards JE, Frye RL, Gensini GG, Gott VL, Griffith LS, et al. A reporting system on patients evaluated for coronary artery disease. Report of the Ad Hoc Committee for Grading of Coronary Artery Disease, Council on Cardiovascular Surgery, American Heart Association. Circulation. 1975; 51:4 Suppl. 5–40.
Article11. Achenbach S, Raggi P. Imaging of coronary atherosclerosis by computed tomography. Eur Heart J. 2010; 31:1442–1448.
Article12. Groothuis JG, Beek AM, Meijerink MR, Brinckman SL, Heymans MW, van Kuijk C, et al. Positive predictive value of computed tomography coronary angiography in clinical practice. Int J Cardiol. 2012; 156:315–319.
Article13. Budoff MJ, Dowe D, Jollis JG, Gitter M, Sutherland J, Halamert E, et al. Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for evaluation of coronary artery stenosis in individuals without known coronary artery disease: results from the prospective multicenter ACCURACY (Assessment by Coronary Computed Tomographic Angiography of Individuals Undergoing Invasive Coronary Angiography) trial. J Am Coll Cardiol. 2008; 52:1724–1732.
Article14. Mowatt G, Cook JA, Hillis GS, Walker S, Fraser C, Jia X, et al. 64-Slice computed tomography angiography in the diagnosis and assessment of coronary artery disease: systematic review and meta-analysis. Heart. 2008; 94:1386–1393.
Article15. Arbab-Zadeh A, Miller JM, Rochitte CE, Dewey M, Niinuma H, Gottlieb I, et al. Diagnostic accuracy of computed tomography coronary angiography according to pre-test probability of coronary artery disease and severity of coronary arterial calcification. The CORE-64 (Coronary Artery Evaluation Using 64-Row Multidetector Computed Tomography Angiography) International Multicenter Study. J Am Coll Cardiol. 2012; 59:379–387.
Article16. Yan RT, Miller JM, Rochitte CE, Dewey M, Niinuma H, Clouse ME, et al. Predictors of inaccurate coronary arterial stenosis assessment by CT angiography. JACC Cardiovasc Imaging. 2013; 6:963–972.
Article17. Kruk M, Noll D, Achenbach S, Mintz GS, Pręgowski J, Kaczmarska E, et al. Impact of coronary artery calcium characteristics on accuracy of CT angiography. JACC Cardiovasc Imaging. 2014; 7:49–58.
Article18. Arbab-Zadeh A, Hoe J. Quantification of coronary arterial stenoses by multidetector CT angiography in comparison with conventional angiography methods, caveats, and implications. JACC Cardiovasc Imaging. 2011; 4:191–202.
Article19. Cademartiri F, Maffei E, Palumbo AA, Malagò R, La Grutta L, Meiijboom WB, et al. Influence of intra-coronary enhancement on diagnostic accuracy with 64-slice CT coronary angiography. Eur Radiol. 2008; 18:576–583.
Article20. Kim C, Hong SJ, Shin DH, Kim JS, Kim BK, Ko YG, et al. Limitations of coronary computed tomographic angiography for delineating the lumen and vessel contours of coronary arteries in patients with stable angina. Eur Heart J Cardiovasc Imaging. 2015; 16:1358–1365.
Article21. Muhlestein JB, Lappé DL, Lima JA, Rosen BD, May HT, Knight S, et al. Effect of screening for coronary artery disease using CT angiography on mortality and cardiac events in high-risk patients with diabetes: the FACTOR-64 randomized clinical trial. JAMA. 2014; 312:2234–2243.
Article22. Douglas PS, Hoffmann U, Patel MR, Mark DB, Al-Khalidi HR, Cavanaugh B, et al. Outcomes of anatomical versus functional testing for coronary artery disease. N Engl J Med. 2015; 372:1291–1300.
Article23. Levine GN, Bates ER, Blankenship JC, Bailey SR, Bittl JA, Cercek B, et al. 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Circulation. 2011; 124:e574–e651.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Evaluation of Myocardial Ischemia Using Coronary Computed Tomography Angiography in Patients with Stable Angina
- Detection of a Left Main Coronary Aneurysm with a Thrombus Presenting as an Acute Myocardial Infarction by Coronary Computed Tomographic Angiography
- A Single Coronary Artery: Right Coronary Artery Originating From the Distal Left Circumflex Artery
- Pathophysiology and Role of Coronary CT Angiography in Stable Angina
- An Unusual Pattern of All Three Coronary Arteries Originating from a Single Coronary Artery Arising from the Right Sinus of Valsalva
