Imaging Findings of Leiomyosarcoma Arising from the Descending Colon Which Presented as a Large Mass in the Retroperitoneum: A Case Report
- Affiliations
-
- 1Department of Radiology, Wonkwang University School of Medicine, Wonkwang University Hospital, Iksan, Korea. yjyh@wonkwang.ac.kr
- 2Department of Pathology, Wonkwang University School of Medicine, Wonkwang University Hospital, Iksan, Korea.
- KMID: 2373960
- DOI: http://doi.org/10.3348/jksr.2017.76.4.245
Abstract
- Leiomyosarcoma is a malignant tumor of smooth muscle cells and it usually originates from the uterus and the retroperitoneum. Leiomyosarcoma of the gastrointestinal tract is rare and leiomyosarcoma of the colon in even more rare, accounting for less than 0.1% of all colonic malignancies. It can be difficult to differentiate leiomyosarcoma from tumor of the retroperitoneum, especially if the mass invades both the colon and the retroperitoneum. We describe the imaging findings of a primary leiomyosarcoma of the descending colon which manifested as a palpable mass in the left lower quadrant of the abdomen and was diagnosed to be of colonic origin by identifying supply vessels of the mass on imaging studies, and the diagnosis was confirmed by surgicopathologic findings.
MeSH Terms
Figure
-
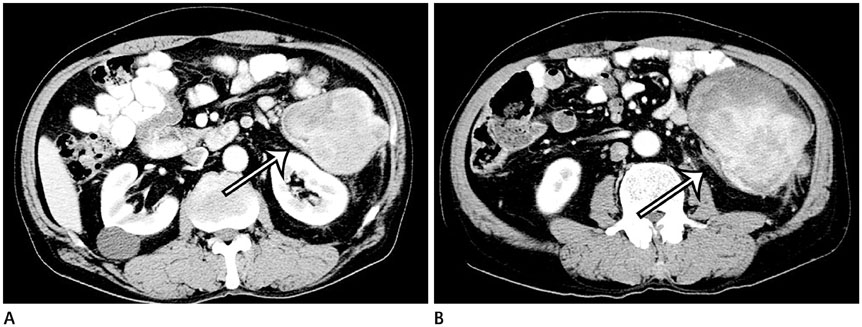
Fig. 1 Abdominal computed tomography (CT) images of colonic leiomyosarcoma in a 69-year-old man. A. CT images reveal a heterogeneously enhancing mass in the left lower quadrant of the abdomen. The lumen of the descending colon is stretched toward the upper portion of the mass, and the wall of the descending colon appears to be embedded in the mass at the contact surface (arrow). These findings represent a positive embedded organ sign. B. The lower portion of the mass compresses the descending colon, which is deformed into a crescent shape (negative embedded organ sign, arrow). The size of the tumor is 13.7 × 9.7 cm.

Fig. 2 Colonoscopic image shows a large, intraluminal protruding mass in the descending colon. The surface of the mass is covered with a whitish exudate.
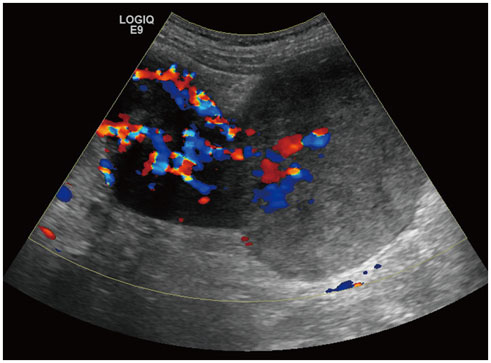
Fig. 3 Ultrasonographic image of colonic leiomyosarcoma. The upper portion of the mass reveals marked hypoechogenicity with greatly increased vascularity, but the lower portion reveals mixed iso- and hypoechogenicity with relatively decreased vascularity compared with the upper portion.

Fig. 4 Magnetic resonance (MR) images of colonic leiomyosarcoma. A. Maximal intensity projection image of contrast-enhanced T1-weighted MR imaging show heterogeneous enhancement of the mass with supply vessels. The mass is supplied by branches of the inferior mesenteric artery (arrowheads). B. On contrast-enhanced T1-weighted coronal MR image, the mass drains into branches of the inferior mesenteric vein (arrowhead). These findings suggest colonic origin of the mass. C. Coronal T2-weighted MR image show a dumbbell shaped mass. The upper portion, which was pathologically proven as conventional leiomyosarcoma, shows heterogeneous low signal intensity (white arrow), whereas the lower portion proven as myxoid leiomyosarcoma shows high signal intensity (black arrow).

Fig. 5 Photograph of the gross pathologic specimen of colonic leiomyosarcoma. A 15 x 20 cm sized hard, well-capsulated dumbbell shaped tumor is noted. The smaller portion shows an intraluminal location, whereas the bigger portion shows an extraluminal location.
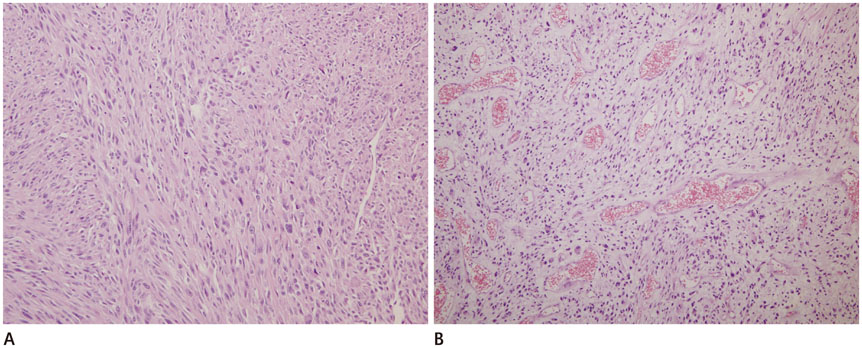
Fig. 6 Photomicrographic images of colonic leiomyosarcoma. A. High power view of the upper portion reveals spindle-shaped cell proliferation combined with mitotic figures compatible with conventional leiomyosarcoma (hematoxylin and eosin, × 200). B. High power view of the lower portion pathologically proven as myxoid leiomyosarcoma shows scattered smooth muscle cells with pleomorphic nuclei within predominantly myxoid stromal cells (hematoxylin and eosin, × 200).
Reference
-
1. Cho SH, Lee JH, Choi SR, Baek YH, Yoon HA, Lee CJ, et al. A case of leiomyosarcoma of the sigmoid colon presenting as intussusception. Korean J Gastrointest Endosc. 2010; 40:270–274.2. Iwasa K, Taniguchi K, Noguchi M, Yamashita H, Kitagawa M. Leiomyosarcoma of the colon presenting as acute suppurative peritonitis. Surg Today. 1997; 27:337–344.3. Ouh YT, Hong JH, Min KJ, So KA, Lee JK. Leiomyosarcoma of the rectum mimicking primary ovarian carcinoma: a case report. J Ovarian Res. 2013; 6:27.4. Warkel RL, Stewart JB, Temple AJ. Leiomyosarcoma of the colon: report of a case and analysis of the relationship of histology to prognosis. Dis Colon Rectum. 1975; 18:501–506.5. O'Sullivan PJ, Harris AC, Munk PL. Radiological imaging features of non-uterine leiomyosarcoma. Br J Radiol. 2008; 81:73–81.6. Lee SH, Ha HK, Byun JY, Kim AY, Cho KS, Lee YR, et al. Radiological features of leiomyomatous tumors of the colon and rectum. J Comput Assist Tomogr. 2000; 24:407–412.7. van den Berg JC, van Heesewijk JP, van Es HW. Malignant stromal tumour of the rectum: findings at endorectal ultrasound and MRI. Br J Radiol. 2000; 73:1010–1012.8. Petscavage-Thomas JM, Walker EA, Logie CI, Clarke LE, Duryea DM, Murphey MD. Soft-tissue myxomatous lesions: review of salient imaging features with pathologic comparison. Radiographics. 2014; 34:964–980.9. Nishino M, Hayakawa K, Minami M, Yamamoto A, Ueda H, Takasu K. Primary retroperitoneal neoplasms: CT and MR imaging findings with anatomic and pathologic diagnostic clues. Radiographics. 2003; 23:45–57.10. Lee WK, Lau EW, Duddalwar VA, Stanley AJ, Ho YY. Abdominal manifestations of extranodal lymphoma: spectrum of imaging findings. AJR Am J Roentgenol. 2008; 191:198–206.
