J Gastric Cancer.
2012 Mar;12(1):49-52.
Late Onset Iatrogenic Diaphragmatic Hernia after Laparoscopy-Assisted Total Gastrectomy for Gastric Cancer
- Affiliations
-
- 1Department of Surgery, College of Medicine, The Catholic University of Korea, Seoul, Korea. kimwook@catholic.ac.kr
Abstract
- Through the advent of surgical techniques and the improvement of laparoscopic tools including the ultrasonic activated scissor, laparoscopic gastrectomy has been increasingly used in far more cases of benign or malignant gastric lesions for the benefit of patients without compromising therapeutic outcomes. Even though possible complications provoked by the ultrasonic activated scissor can be prevented during the procedure with increasing advanced laparoscopic experience and supervision, unexpected late complications after the operations rarely occur. An extremely rare case of left incarcerated diaphragmatic hernia of the transverse colon developed in an 81-year-old female patient as a late complication, 8 months after laparoscopy-assisted total gastrectomy for gastric cancer, with laparoscopy successfully resumed and without the need to sacrifice any portion of the bowel.
Keyword
MeSH Terms
Figure
-
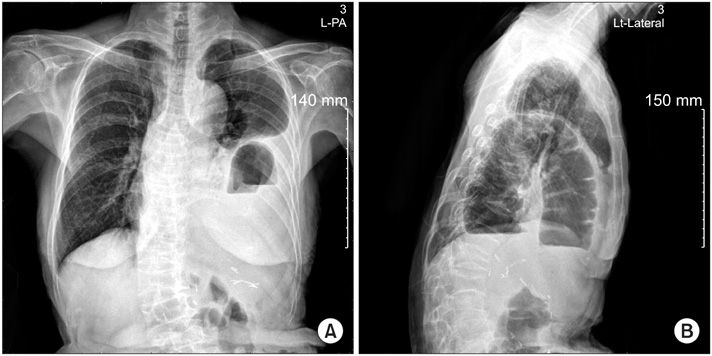
Fig. 1 (A, B) Preoperative plain chest film showed air-fluid levels by the herniated bowels in the left pleural cavity.
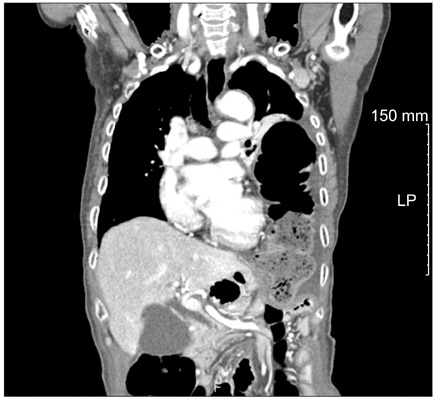
Fig. 2 Coronal section of the chest computed tomogram showed herniated bowels definitely in the left pleural cavity preoperatively.
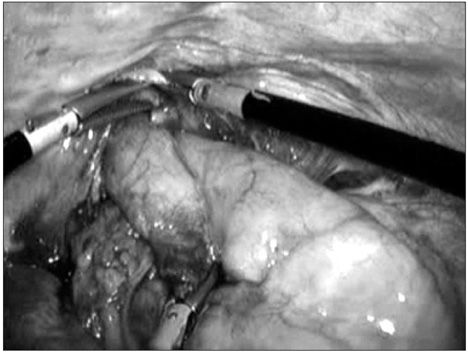
Fig. 3 Herniated transverse colon was retrieved through the diaphragmatic defect by laparoscopically.
Reference
-
1. Shehzad K, Mohiuddin K, Nizami S, Sharma H, Khan IM, Memon B, et al. Current status of minimal access surgery for gastric cancer. Surg Oncol. 2007. 16:85–98.
Article2. Farn J, Hammerman AM, Brunt LM. Intraoperative pneumothorax during laparoscopic cholecystectomy: a complication of prior transdiaphragmatic surgery. Surg Laparosc Endosc. 1993. 3:219–222.3. Eder F, Putzki H, Tautenhahn E. Right-sided pneumothorax in laparoscopic cholecystectomy. Chirurg. 1994. 65:484–485.4. Armstrong PA, Miller SF, Brown GR. Diaphragmatic hernia seen as a late complication of laparoscopic cholecystectomy. Surg Endosc. 1999. 13:817–818.
Article5. Kent MS, Luketich JD, Tsai W, Churilla P, Federle M, Landreneau R, et al. Revisional surgery after esophagectomy: an analysis of 43 patients. Ann Thorac Surg. 2008. 86:975–983.
Article6. Vallböhmer D, Hölscher AH, Herbold T, Gutschow C, Schröder W. Diaphragmatic hernia after conventional or laparoscopic-assisted transthoracic esophagectomy. Ann Thorac Surg. 2007. 84:1847–1852.
Article7. Kim JJ, Song KY, Chin HM, Kim W, Jeon HM, Park CH, et al. Totally laparoscopic gastrectomy with various types of intracorporeal anastomosis using laparoscopic linear staplers: preliminary experience. Surg Endosc. 2008. 22:436–442.
Article8. Besozzi A, Besozzi S, Lanza V, Mitolo CI, Novelli D, Sisto T. Laparoscopic treatment gastric cancer with advanced techniques: technical notes and follow-up. Chir Ital. 2007. 59:63–67.9. Balázs A, Forgács A, Flautner L, Kupcsulik P. A case of unusual complication of diaphragmatic herniation of transverse colon following transhiatal esophagectomy. Orv Hetil. 1997. 138:2535–2538.10. Aly A, Watson DI. Diaphragmatic hernia after minimally invasive esophagectomy. Dis Esophagus. 2004. 17:183–186.
Article11. Kuhn R, Schubert D, St Wolff, Marusch F, Lippert H, Pross M. Repair of diaphragmatic rupture by laparoscopic implantation of a polytetrafluoroethylene patch. Surg Endosc. 2002. 16:1495.
Article12. Killeen KL, Mirvis SE, Shanmuganathan K. Helical CT of diaphragmatic rupture caused by blunt trauma. AJR Am J Roentgenol. 1999. 173:1611–1616.
Article13. Kaya SO, Karabulut N, Yuncu G, Sevinc S, Kiroğlu Y. Sinus cut-off sign: a helpful sign in the CT diagnosis of diaphragmatic rupture associated with pleural effusion. Eur J Radiol. 2006. 59:253–256.
Article14. Matthews BD, Bui H, Harold KL, Kercher KW, Adrales G, Park A, et al. Laparoscopic repair of traumatic diaphragmatic injuries. Surg Endosc. 2003. 17:254–258.
Article15. Murray JA, Demetriades D, Asensio JA, Cornwell EE 3rd, Velmahos GC, Belzberg H, et al. Occult injuries to the diaphragm: prospective evaluation of laparoscopy in penetrating injuries to the left lower chest. J Am Coll Surg. 1998. 187:626–630.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Occurrence of iatrogenic pneumothorax during laparoscopy-assisted distal gastrectomy: A case report
- Laparoscopy-Assisted Distal Gastrectomy for Early Gastric Cancer in the Elderly
- Non-Randomized Confirmatory Trial of Laparoscopy-Assisted Total Gastrectomy and Proximal Gastrectomy with Nodal Dissection for Clinical Stage I Gastric Cancer: Japan Clinical Oncology Group Study JCOG1401
- The Preservation of Left Gastric Atery in Laparoscopy-Assisted Subtotal Gastrectomy with Splenectomy of Stomach Cancer
- Laparoscopy-assisted Total Gastrectomy with Pancreas-preserving Splenectomy for Early Gastric Cancer: A Case Report
