Clinical Characteristics of Intraorbital Foreign Bodies: Our Experience with 14 Cases
- Affiliations
-
- 1Department of Ophthalmology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. lineblue@hanmail.net
- 2Department of Ophthalmology, Ilsan Paik Hospital, Inje University College of Medicine, Goyang, Korea.
- KMID: 2371904
- DOI: http://doi.org/10.3341/jkos.2017.58.3.251
Abstract
- PURPOSE
To evaluate the clinical characteristics of intraorbital foreign bodies as well as the treatment outcomes.
METHODS
This was a noncomparative interventional case series. Clinical data and radiographic images were gathered via retrospective chart reviews of 14 patients who underwent surgical removal of intraorbital foreign bodies by an oculoplastic surgeon at the Asan Medical Center, Seoul, Korea between July 2012 and November 2015.
RESULTS
The mean age of patients was 45.1 years and 13 patients (92.9%) were male. There were 9 metallic; 3 nonmetallic, inorganic; and 2 organic intraorbital foreign bodies in this series. The most common orbital complication was orbital wall fracture (8, 57.1%), and one patient had orbital cellulitis associated with a wooden foreign body. Six patients (42.9%) underwent surgical removal of foreign bodies in a delayed setting, and 4 of them needed surgery to allow for the brain magnetic resonance image tests to evaluate neurologic problems. There were 6 patients (42.9%) who had a postoperative corrected visual acuity worse than 20/200, and all of them had poor visual acuity at the time of injury due to associated eyeball or optic nerve injuries. Four patients (28.6%) had eyeball movement limitations from the initial trauma, but only 1 patient had persistent limitations postoperatively. There were no other complications associated with surgical removal.
CONCLUSIONS
The majority of patients with intraorbital foreign bodies were male who had periorbital traumas. The most common foreign body was metal, and orbital wall fractures were common. The poor visual prognosis was related to the eyeball or optic nerve injuries from the initial trauma. The urgent surgical removal should be performed for organic foreign bodies or associated orbital/ocular injuries. Metallic foreign bodies may also be considered for removal to allow for possible brain magnetic resonance image evaluations in the future.
Keyword
MeSH Terms
Figure
-
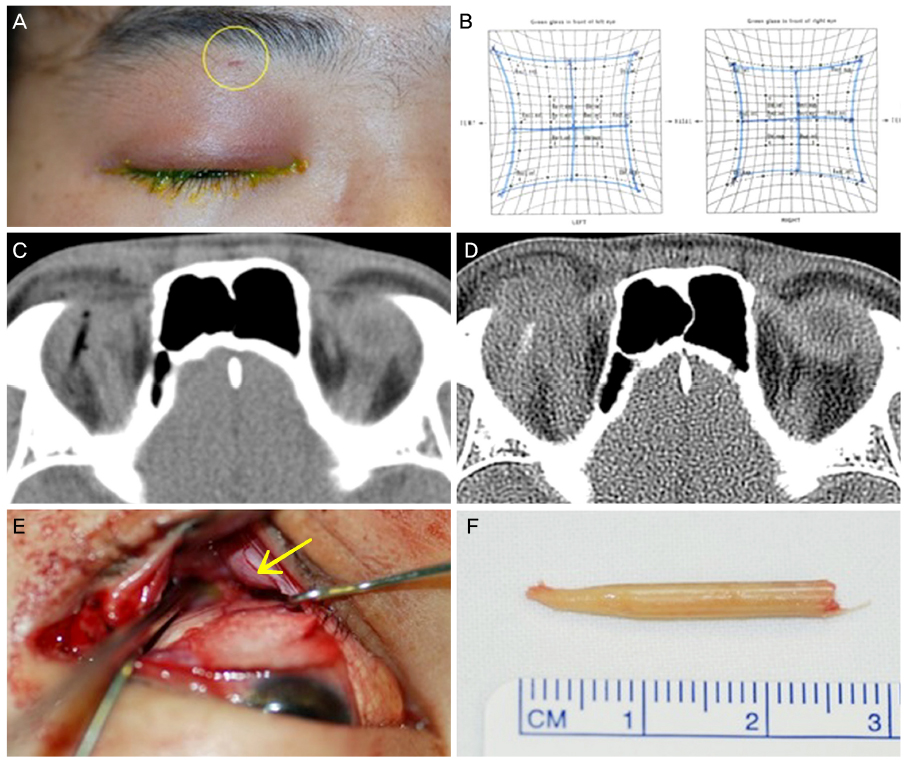
Figure 1 A case of orbital wooden foreign body. (A) A 30-year-old male patient was seen with a right upper lid swelling and ptosis which developed 3 days after periorbital trauma. He was punched under the influence of alcohol 4 days earlier. He visited another hospital, but intraorbital foreign body was not detected at that time. The entrance wound was found just below the brow (yellow circle). (B) A Hess screening test revealed mild ocular movement limitation in upgaze in the right eye resulting a vertical diplopia. (C) An axial computed tomography (CT) scan at the time of the injury showed a linear radiolucent lesion in the right superior orbit, which was misdiagnosed as intraorbital air at another hospital. (D) Follow-up CT scan 4 days after the injury revealed the corresponding lesion became to have a high attenuating density and surrounding inflammation. (E) Surgical exploration through a transconjunctival approach revealed a wooden stick foreign body (yellow arrow). (F) A removed wooden foreign body.
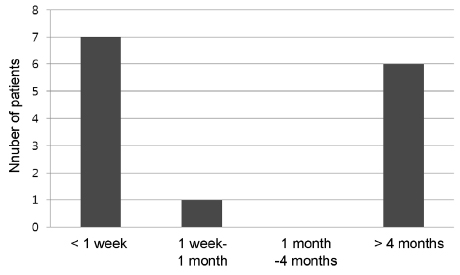
Figure 2 Time interval between the injury and the surgical removal. Seven patients (50%) underwent surgical removal within a week, but six patients (42.9%) received delayed surgery more than four months after trauma.
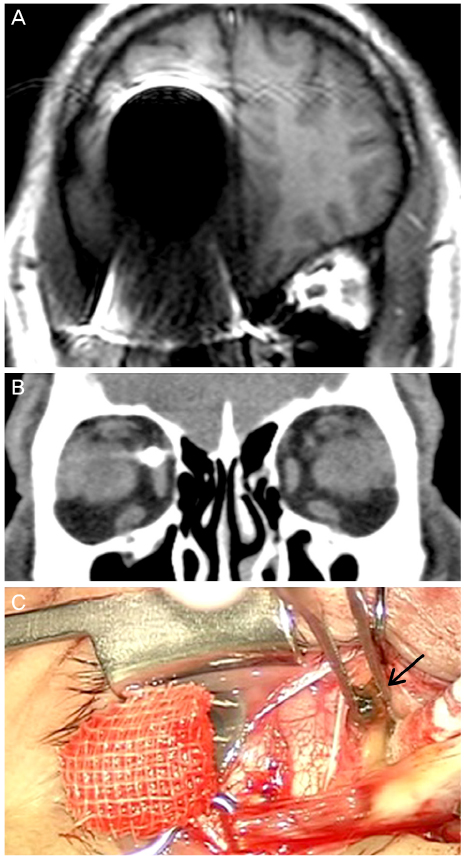
Figure 3 A case of orbital metal foreign body. (A) A 58-year-old man was seen with an incidental detection of metallic foreign body during a neurologic workup for an episode of syncope 1 month earlier. A magnetic resonance image showed a significant artifact caused by a metallic foreign body in the right orbit. He had a trauma history while gardening with a grass cutter 8 years earlier. (B) A coronal computed tomography scan showed a metallic foreign body in the right superonasal orbit adjacent to the medial rectus muscle. (C) A piece of rusty iron (black arrow) which was well encapsulated was removed through a limbal conjunctival incision.
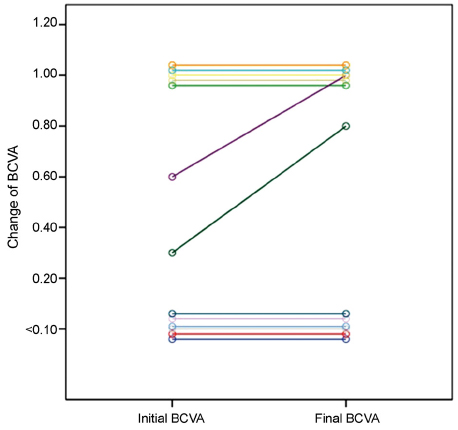
Figure 4 Linear chart comparing the initial and the final best corrected visual acuities (Snellen visual acuity) of 13 patients with intraorbital foreign bodies. One patient was not evaluated for the visual acuity at the initial visit because he was under the influence of alcohol. BCVA = best corrected visual acuity.
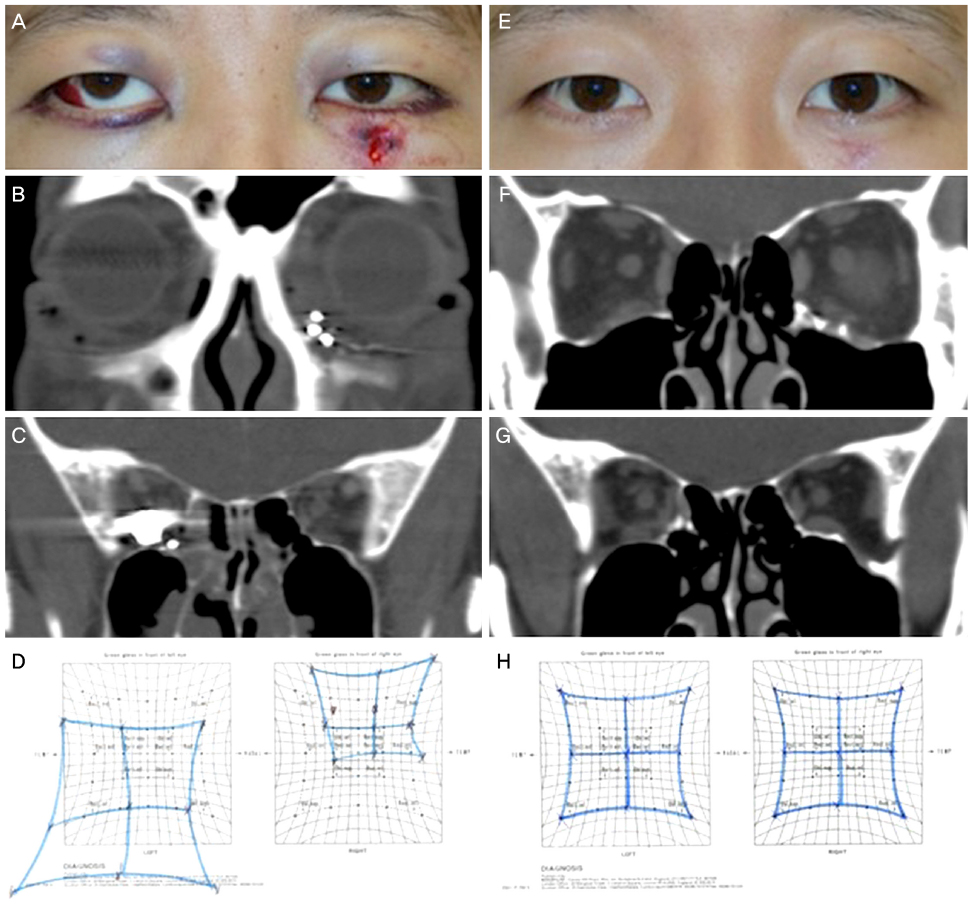
Figure 5 A case of orbital gunshot injury. (A) A 28-year-old man had a gunshot injury. The bullet penetrated the left forearm, left face, and the right orbit. His vision was 20/25 in the right eye, and he had hypertropia and exotropia. (B, C) Computed tomography (CT) scans revealed the penetrating tract along the left cheek, left inferior orbit, ethmoid sinus, and the right posterior orbit. There were multiple pieces of shrapnel in the right orbit, and the main metallic foreign body of bullet was in the right orbital apex. (D) He had a significant eyeball movement limitation at the initial examination. (E) Surgery was successfully performed to remove the intraorbital bullet and multiple metal pieces, and the left orbital floor fracture was repaired. Intraoperative C-arm x-ray system w as used to confirm the complete removal of foreign bodies. One month after surgery, the best corrected visual acuity was 20/20 in his right eye, and he showed orthophoria. (F, G) Follow-up CT scans demonstrated the well-reconstructed right orbital floor without shrapnel, and the complete removal of bullet foreign body from the right orbital apex. (H) Follow-up Hess screen test showed no eyeball movement limitation.
Reference
-
1. Kim HK, Chung WS. Clinical experience of intraorbital foreign body. J Korean Ophthalmol Soc. 1997; 38:177–184.2. Fulcher TP, McNab AA, Sullivan TJ. Clinical features and management of intraorbital foreign bodies. Ophthalmology. 2002; 109:494–500.3. Finkelstein M, Legmann A, Rubin PA. Projectile metallic foreign bodies in the orbit: a retrospective study of epidemiologic factors, management, and outcomes. Ophthalmology. 1997; 104:96–103.4. Nasr AM, Haik BG, Fleming JC, et al. Penetrating orbital injury with organic foreign bodies. Ophthalmology. 1999; 106:523–532.5. Cartwright MJ, Kurumety UR, Frueh BR. Intraorbital wood foreign body. Ophthal Plast Reconstr Surg. 1995; 11:44–48.6. Scharf J, Zonis S. Proptosis as presenting symptom of orbital foreign body. J Pediatr Ophthalmol. 1977; 14:176–177.7. Bullock JD, Warwar RE, Bartley GB, et al. Unusual orbital foreign bodies. Ophthal Plast Reconstr Surg. 1999; 15:44–51.8. Karcioglu ZA, Nasr AM. Diagnosis and management of orbital inflammation and infections secondary to foreign bodies: a clinical review. Orbit. 1998; 17:247–269.9. Macrae JA. Diagnosis and management of a wooden orbital foreign body: case report. Br J Ophthalmol. 1979; 63:848–851.10. Wang WJ, Li CX, Sebag J, Ni C. Orbital fistula. Causes and treatment of 20 cases. Arch Ophthalmol. 1983; 101:1721–1723.11. Charteris DG. Posterior penetrating injury of the orbit with retained foreign body. Br J Ophthalmol. 1988; 72:432–433.12. Pinto A, Brunese L, Daniele S, et al. Role of computed tomography in the assessment of intraorbital foreign bodies. Semin Ultrasound CT MR. 2012; 33:392–395.13. Howe L, Jones NS. Guidelines for the management of periorbital cellulitis/abscess. Clin Otolaryngol Allied Sci. 2004; 29:725–728.14. Michon J, Liu D. Intraorbital foreign bodies. Semin Ophthalmol. 1994; 9:193–199.15. Kim ST, Kim DH. A case of intraorbital foreign body after gunshot wounds. J Korean Ophthalmol Soc. 2009; 50:649–655.16. Lim JH, Kwak MS. Case report of retained intraorbital metallic foreign body removal. J Korean Ophthalmol Soc. 1999; 40:1127–1132.17. Ho VH, Wilson MW, Fleming JC, Haik BG. Retained intraorbital metallic foreign bodies. Ophthal Plast Reconstr Surg. 2004; 20:232–236.18. Roden D, Cleary P, Eustace P. A five-year survey of ocular shotgun injuries in Ireland. Br J Ophthalmol. 1987; 71:449–453.19. Yang SW, Kim YD, Kim KR. A case of retained multiple intraorbital foreign bodies. J Korean Ophthalmol Soc. 2004; 45:1380–1385.20. Jang JH, Kim BJ. Two cases of intraorbital wooden foreign bodies. J Korean Ophthalmol Soc. 2004; 45:691–698.21. Liu D, Al Shail E. Retained orbital wooden foreign body: a surgical technique and rationale. Ophthalmology. 2002; 109:393–399.22. Kelly WM, Paglen PG, Pearson JA, et al. Ferromagnetism of intraocular foreign body causes unilateral blindness after MR study. AJNR Am J Neuroradiol. 1986; 7:243–245.
