Wiring Techniques for the Fixation of Trochanteric Fragments during Bipolar Hemiarthroplasty for Femoral Intertrochanteric Fracture: Clinical Study and Technical Note
- Affiliations
-
- 1Department of Orthopaedic Surgery, CHA Bundang Medical Center, CHA University, Seongnam, Korea. drjmlee@naver.com
- KMID: 2371767
- DOI: http://doi.org/10.5371/hp.2017.29.1.44
Abstract
- PURPOSE
Femoral intertrochanteric fractures are common in the elderly. Appropriate surgical fixation of trochanteric fracture fragments can restore normal anatomical structure and ambulation, and can aid in the recovery of biomechanical function of the hip. We evaluated clinical outcomes of bipolar hemiarthroplasty using a wiring technique for trochanteric fracture fragment fixation.
MATERIALS AND METHODS
From September 2006 to February 2015, a total of 260 cases underwent simultaneous bipolar hemiarthroplasty and wire fixation. A total of 65 patients (69 hips) with an average age of 78 years and more than one year of follow-up was included in the study. Using pre-, postoperative and follow-up radiograms, we evaluated wire fixation failure and also assessed changes in walking ability.
RESULTS
Loosening or osteolysis around the stem was not observed; however, we did observe bone growth around the stem (54 cases), cortical hypertrophy (6 cases), a wide range of sclerotic lines but no stem subsidence (1 case), wire breakage (9 cases), and fracture fragment migration with no significant functional deficiency (2 cases).
CONCLUSION
Our study showed that additional wiring for trochanteric fracture fragment fixation following bipolar hemiarthroplasty can help restore normal anatomy. The added stability results in faster rehabilitation, and good clinical and radiographic outcomes. We recommend this procedure in this type of fracture.
Keyword
MeSH Terms
Figure
-
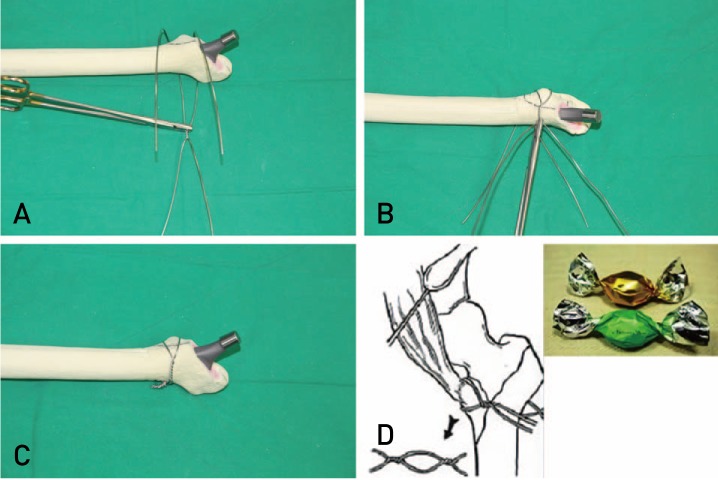
Fig. 1 (A) This wiring is performed before insertion of prosthesis components. Each wire is inserted into the superior and inferior aspects of the displaced lesser trochanter and wire knots are placed at the posterior aspect of the bone fragment. (B) Hip prosthesis insertion is conducted after making bone fragments movable with the wires by fixing them using knots anteriorly. (C) After inserting all hip prostheses, lesser trochanteric fragments are reduced using wires and fixed by making knots laterally. (D) A schematic diagram representing the relationship of lesser trochanteric fragments and the iliopsoas, and candy package wiring (named because wiring shape resembles a candy package).
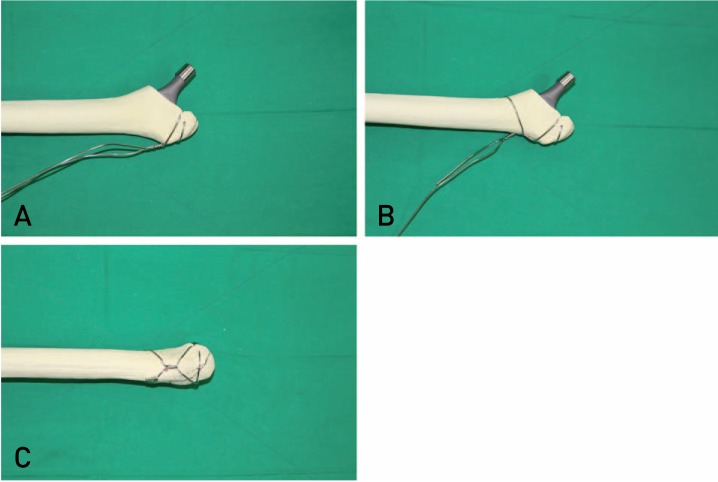
Fig. 2 (A) To enhance rigidity of fixation, a 1.5-mm wire was tied two or three times transversely over the greater trochanter and knots are made laterally. Tying the wire using holes drilled into the anterior portion of greater trochanter can add the additional stability. (B) After making the primary knot, the wire is tightened to the inferior to the lesser trochanter. (C) After tying the wire below the lesser trochanter, the secondary knot is made at the lateral aspect.
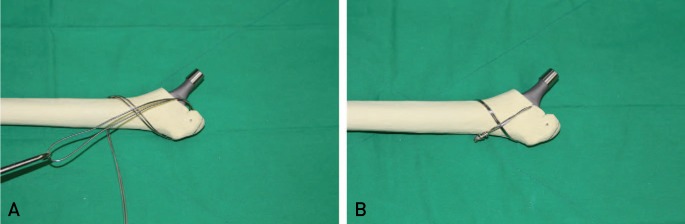
Fig. 3 (A) A double-strand wire is tied to the greater and lesser trochanters using a figure-8 wiring. (B) A wire knot is made rigidly at the lateral aspect. Using this wiring method, fixation can be accomplished by adjusting the position of wires depending on the pattern and location of fracture lines.
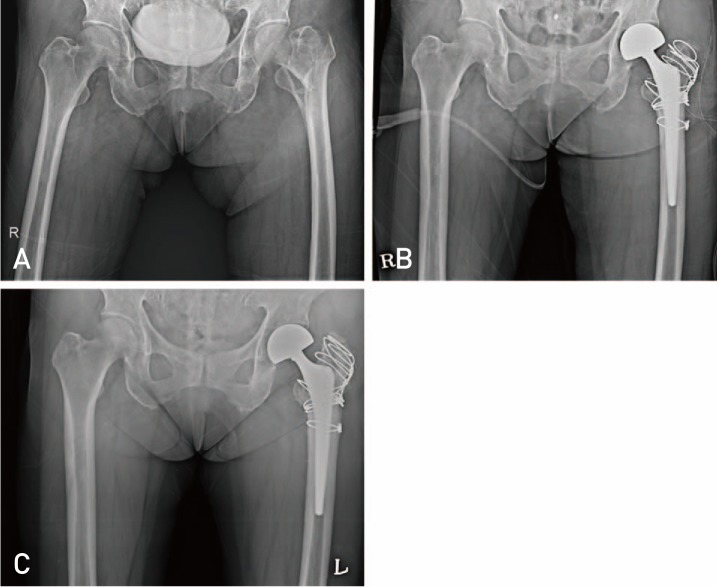
Fig. 4 (A) A 72-year old female patient visited our hospital due to intertrochanteric fracture of left femur after fall down from a height of 1 m. (Preoperative Clawson's Ambulation Capacity: Class 4). (B) Images after performing bipolar hemiarthroplasty and wiring fixation (transverse wiring with distal pulling wire ×2, candy-package wiring). (C) Postoperative 1-year follow-up; no limping gait, restoration of pre-injury ambulatory ability (Clawson's Classification: Class 4) and radiological signs of bone union.
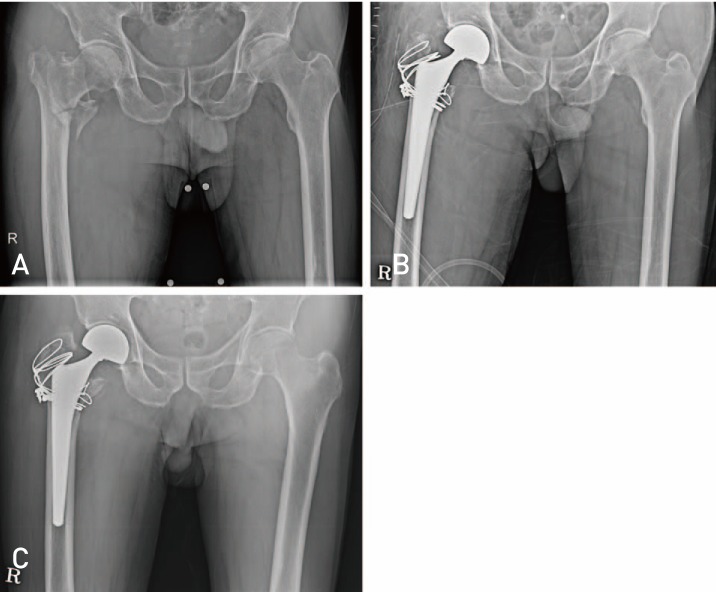
Fig. 5 (A) An 88-year old male patient visited our hospital due to intertrochanteric fracture of right femur after slip down on the way to the toilet. (Preoperative Clawson's Ambulation Capacity: Class 3). (B) Images after performing bipolar hemiarthroplasty and wiring fixation (transverse wiring with distal pulling wire, figure-8 wiring, candy package wiring). (C) Postoperative 1-year follow-up; restoration of pre-injury ambulatory ability (Clawson's Classification: Class 3) and radiological signs of bone union despite slight displacement.
Cited by 2 articles
-
Fixation of Trochanteric Fragments in Cementless Bipolar Hemiarthroplasty of Unstable Intertrochanteric Fracture: Cerclage Wiring
Young-Kyun Lee, Chan Ho Park, Kyung-Hoi Koo
Hip Pelvis. 2017;29(4):262-269. doi: 10.5371/hp.2017.29.4.262.Hip Arthroplasty Using the Bencox® Hip System: An Evaluation of a Consecutive Series of One Thousand Cases
Joong-Myung Lee, Young-Suk Sim, Dae-Sung Choi
Hip Pelvis. 2018;30(4):210-218. doi: 10.5371/hp.2018.30.4.210.
Reference
-
1. Kyle RF, Gustilo RB, Premer RF. Analysis of six hundred and twenty-two intertrochanteric hip fractures. J Bone Joint Surg Am. 1979; 61:216–221. PMID: 422605.
Article2. Haentjens P, Casteleyn PP, De Boeck H, Handelberg F, Opdecam P. Treatment of unstable intertrochanteric and subtrochanteric fractures in elderly patients. Primary bipolar arthroplasty compared with internal fixation. J Bone Joint Surg Am. 1989; 71:1214–1225. PMID: 2777850.
Article3. Lu-Yao GL, Keller RB, Littenberg B, Wennberg JE. Outcomes after displaced fractures of the femoral neck. A meta-analysis of one hundred and six published reports. J Bone Joint Surg Am. 1994; 76:15–25. PMID: 8288658.
Article4. Hardy DC, Descamps PY, Krallis P, et al. Use of an intramedullary hip-screw compared with a compression hip-screw with a plate for intertrochanteric femoral fractures. A prospective, randomized study of one hundred patients. J Bone Joint Surg Am. 1998; 80:618–630. PMID: 9611022.
Article5. Kim WY, Han CH, Park JI, Kim JY. Failure of intertrochanteric fracture fixation with a dynamic hip screw in relation to pre-operative fracture stability and osteoporosis. Int Orthop. 2001; 25:360–362. PMID: 11820441.
Article6. Rodop O, Kiral A, Kaplan H, Akmaz I. Primary bipolar hemiprosthesis for unstable intertrochanteric fractures. Int Orthop. 2002; 26:233–237. PMID: 12185526.
Article7. Kayali C, Agus H, Ozluk S, Sanli C. Treatment for unstable intertrochanteric fractures in elderly patients: internal fixation versus cone hemiarthroplasty. J Orthop Surg (Hong Kong). 2006; 14:240–244. PMID: 17200522.
Article8. Green S, Moore T, Proano F. Bipolar prosthetic replacement for the management of unstable intertrochanteric hip fractures in the elderly. Clin Orthop Relat Res. 1987; (224):169–177.
Article9. McGrory BJ, Morrey BF, Cahalan TD, An KN, Cabanela ME. Effect of femoral offset on range of motion and abductor muscle strength after total hip arthroplasty. J Bone Joint Surg Br. 1995; 77:865–869. PMID: 7593096.
Article10. Bourne RB, Rorabeck CH. Soft tissue balancing: the hip. J Arthroplasty. 2002; 17(4 Suppl 1):17–22. PMID: 12068397.
Article11. Lee JM, Lee JH, Lee CW, Kim HM. New wiring method for lesser trochanter fixation in unstable intertrochanteric dractures: technical note. J Korean Fract Soc. 2005; 18:209–212.12. Jin WJ, Dai LY, Cui YM, Zhou Q, Jiang LS, Lu H. Reliability of classification systems for intertrochanteric fractures of the proximal femur in experienced orthopaedic surgeons. Injury. 2005; 36:858–861. PMID: 15949488.
Article13. Anglen JO, Weinstein JN. Nail or plate fixation of intertrochanteric hip fractures: changing pattern of practice. A review of the American Board of Orthopaedic Surgery Database. J Bone Joint Surg Am. 2008; 90:700–707. PMID: 18381305.14. Aros B, Tosteson AN, Gottlieb DJ, Koval KJ. Is a sliding hip screw or im nail the preferred implant for intertrochanteric fracture fixation? Clin Orthop Relat Res. 2008; 466:2827–2832. PMID: 18465180.
Article15. Kim SY, Kim YG, Hwang JK. Cementless calcar-replacement hemiarthroplasty compared with intramedullary fixation of unstable intertrochanteric fractures. A prospective, randomized study. J Bone Joint Surg Am. 2005; 87:2186–2192. PMID: 16203881.16. Lee YK, Ha YC, Chang BK, Kim KC, Kim TY, Koo KH. Cementless bipolar hemiarthroplasty using a hydroxyapatite-coated long stem for osteoporotic unstable intertrochanteric fractures. J Arthroplasty. 2011; 26:626–632. PMID: 20637559.
Article17. Masonis JL, Bourne RB. Surgical approach, abductor function, and total hip arthroplasty dislocation. Clin Orthop Relat Res. 2002; (405):46–53. PMID: 12461355.
Article18. Mukka S, Lindqvist J, Peyda S, et al. Dislocation of bipolar hip hemiarthroplasty through a postero-lateral approach for femoral neck fractures: a cohort study. Int Orthop. 2015; 39:1277–1282. PMID: 25557759.
Article19. Lim YW, Chang YJ, Kwon SY, Kim YS. A simple method using a PACS to minimize leg length discrepancy in primary THA: a method to minimize leg length discrepancy. J Arthroplasty. 2013; 28:1791–1795. PMID: 23540533.20. Chan KC, Gill GS. Cemented hemiarthroplasties for elderly patients with intertrochanteric fractures. Clin Orthop Relat Res. 2000; (371):206–215.
Article21. von Roth P, Abdel MP, Harmsen WS, Berry DJ. Cemented bipolar hemiarthroplasty provides definitive treatment for femoral neck fractures at 20 years and beyond. Clin Orthop Relat Res. 2015; 473:3595–3599. PMID: 26186915.
Article22. Hong CC, Nashi N, Makandura MC, Krishna L. Cemented hemiarthroplasty in traumatic displaced femoral neck fractures and deep vein thrombosis: is there really a link? Singapore Med J. 2016; 57:69–72. PMID: 26892829.
Article23. Qi X, Zhang Y, Pan J, Ma L, Wang L, Wang J. Effect of bone cement implantation on haemodynamics in elderly patients and preventive measure in cemented hemiarthroplasty. Biomed Res Int. 2015; 2015:568019. PMID: 26413535.
Article24. Lee JM, Nam HT, Lee SH. Bipolar hemiarthroplasty with cementless femoral stem for unstable intertrochanteric fractures. J Korean Orthop Assoc. 2012; 47:79–85.
Article25. Lee JM, Jeon JB. Result of a minimum five-year follow-up of hip arthroplasty using the Bencox(R) hip stem. J Korean Orthop Assoc. 2014; 49:126–132.26. Amstutz HC, Mai LL, Schmidt I. Results of interlocking wire trochanteric reattachment and technique refinements to prevent complications following total hip arthroplasty. Clin Orthop Relat Res. 1984; (183):82–89.
Article27. Barrack RL, Butler RA. Current status of trochanteric reattachment in complex total hip arthroplasty. Clin Orthop Relat Res. 2005; 441:237–242. PMID: 16331009.
Article28. Koyama K, Higuchi F, Kubo M, Okawa T, Inoue A. Reattachment of the greater trochanter using the Dall-Miles cable grip system in revision hip arthroplasty. J Orthop Sci. 2001; 6:22–27. PMID: 11289581.
Article29. Kim WY, Han CH, Ji JH, Kim YY, Lee KS, Lee SW. Fixation for reattachment of trochanteric fragment in pertrochanteric fracture treated with bipolar hemiarthroplasty. J Korean Hip Soc. 2006; 18:67–72.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Fixation of Trochanteric Fragments in Cementless Bipolar Hemiarthroplasty of Unstable Intertrochanteric Fracture: Cerclage Wiring
- Bipolar Hemiarthroplasty in Unstable Intertrochanteric Fractures with an Effective Wiring Technique
- Comparison between the Methods for Fixation of Greater Trochanteric Fragment in Cemented Bipolar Hemiarthroplasty for Unstable Intertrochanteric Fracture
- Fixation for Reattachment of Trochanteric Fragment in Pertrochanteric Fracture Treated with Bipolar Hemiarthroplasty
- Trochanteric Management for Unstable Intertrochanteric Femoral Fracture in the Elderly Patients
