Anesth Pain Med.
2017 Jan;12(1):62-67. 10.17085/apm.2017.12.1.62.
Development of atrial flutter after induction of general anesthesia and conversion to atrial fibrillation: A case report
- Affiliations
-
- 1Department of Anesthesiology and Pain Medicine, Kwangju Christian Hospital, Gwangju, Korea. eusuk@medigate.net
- 2Department of Anesthesiology and Pain Medicine, KS Hospital, Gwangju, Korea.
- KMID: 2369669
- DOI: http://doi.org/10.17085/apm.2017.12.1.62
Abstract
- The most frequent perioperative cardiovascular event is cardiac dysrhythmia, defined as an abnormality of cardiac rate, rhythm or conduction. Although the occurrence of arrhythmia during the perioperative period is not uncommon, a case of newly developed perioperative atrial flutter which spontaneously converts to atrial fibrillation is rare. We report a case of atrial flutter that developed immediately after induction of general anesthesia, in a 70-year-old male patient who previously had a normal sinus rhythm. Atrial flutter changed spontaneously to atrial fibrillation after discharge to the recovery room. Dysrhythmia was unresponsive to drug therapy, and the atrial fibrillation disappeared after electric cardioversion.
MeSH Terms
Figure
-

Fig. 1 Electrocardiogram taken one day before surgery. Regular sinus rhythm without arrhythmia was observed.

Fig. 2 Monitoring screen with lead II electrocardiography during anesthesia in operating room.

Fig. 3 Electrocardiogram taken immediately after arrival at recovery room. Atrial flutter with 2:1 atrioventricular block and saw-toothed P wave was observed.
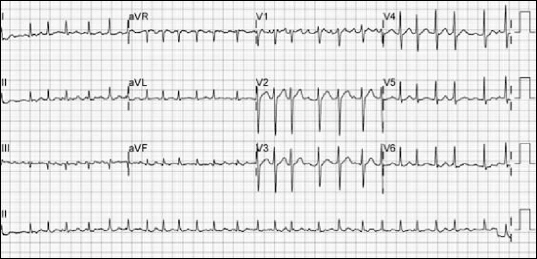
Fig. 4 Electrocardiogram before electric cardioversion. Atrial flutter changed to atrial fibrillation with rapid ventricular responses (ventricular rate: 160–170 bpm).
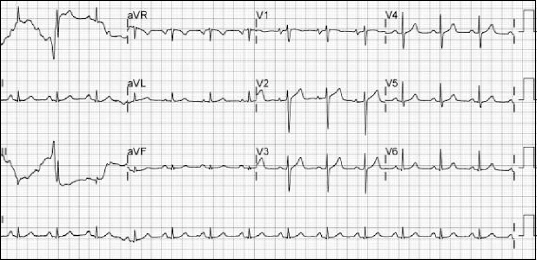
Fig. 5 Electrocardiogram after electric DC cardioversion. Regular sinus rhythm was restored.
Reference
-
1. Kwak HJ, Lee KC, Lee D, Kim HS, Kim SH. Atrial flutter associated with high pressure pneumoperitoneum during laparoscopic gastrectomy: A case report. Anesth Pain Med. 2010; 5:67–9.2. Ortiz J, Niwano S, Abe H, Rudy Y, Johnson NJ, Waldo AL. Mapping the conversion of atrial flutter to atrial fibrillation and atrial fibrillation to atrial flutter. Insights into mechanisms. Circ Res. 1994; 74:882–94. DOI: 10.1161/01.RES.74.5.882. PMID: 8156635.3. Roithinger FX, Karch MR, Steiner PR, SippensGroenewegen A, Lesh MD. Relationship between atrial fibrillation and typical atrial flutter in humans: activation sequence changes during spontaneous conversion. Circulation. 1997; 96:3484–91. DOI: 10.1161/01.CIR.96.10.3484. PMID: 9396445.4. Naccarelli GV, Varker H, Lin J, Schulman KL. Increasing prevalence of atrial fibrillation and flutter in the United States. Am J Cardiol. 2009; 104:1534–9. DOI: 10.1016/j.amjcard.2009.07.022. PMID: 19932788.5. Christians KK, Wu B, Quebbeman EJ, Brasel KJ. Postoperative atrial fibrillation in noncardiothoracic surgical patients. Am J Surg. 2001; 182:713–5. DOI: 10.1016/S0002-9610(01)00799-1.6. Amar D. Perioperative atrial tachyarrhythmias. Anesthesiology. 2002; 97:1618–23. DOI: 10.1097/00000542-200212000-00039. PMID: 12459693.7. Wen ZC, Chen SA, Tai CT, Huang JL, Chang MS. Role of autonomic tone in facilitating spontaneous onset of typical atrial flutter. J Am Coll Cardiol. 1998; 31:602–7. DOI: 10.1016/S0735-1097(97)00555-X.8. Lampert R, Shusterman V, Burg MM, Lee FA, Earley C, Goldberg A, et al. Effects of psychologic stress on repolarization and relationship to autonomic and hemodynamic factors. J Cardiovasc Electrophysiol. 2005; 16:372–7. DOI: 10.1046/j.1540-8167.2005.40580.x. PMID: 15828878.9. Maurice-Szamburski A, Auquier P, Viarre-Oreal V, Cuvillon P, Carles M, Ripart J, et al. Effect of sedative premedication on patient experience after general anesthesia: a randomized clinical trial. JAMA. 2015; 313:916–25. DOI: 10.1001/jama.2015.1108. PMID: 25734733.10. Emori T, Fukushima K, Saito H, Nakayama K, Ohe T. Atrial electrograms and activation sequences in the transition between atrial fibrillation and atrial flutter. J Cardiovasc Electrophysiol. 1998; 9:1173–9. DOI: 10.1111/j.1540-8167.1998.tb00089.x. PMID: 9835261.11. Hsieh MH, Tai CT, Tsai CF, Yu WC, Lin WS, Huang JL, et al. Mechanism of spontaneous transition from typical atrial flutter to atrial fibrillation: role of ectopic atrial fibrillation foci. Pacing Clin Electrophysiol. 2001; 24:46–52. DOI: 10.1046/j.1460-9592.2001.00046.x. PMID: 11227968.12. Waldo AL, Feld GK. Inter-relationships of atrial fibrillation and atrial flutter mechanisms and clinical implications. J Am Coll Cardiol. 2008; 51:779–86. DOI: 10.1016/j.jacc.2007.08.066. PMID: 18294560.13. January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC Jr, et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol. 2014; 64:e1–76. DOI: 10.1016/j.jacc.2014.03.022. PMID: 24685669.14. Dahl V, Pendeville PE, Hollmann MW, Heier T, Abels EA, Blobner M. Safety and efficacy of sugammadex for the reversal of rocuronium-induced neuromuscular blockade in cardiac patients undergoing noncardiac surgery. Eur J Anaesthesiol. 2009; 26:874–84. DOI: 10.1097/EJA.0b013e32832c605b. PMID: 19455040.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Electrophysiologic Characteristics in the Process of Conversion from Atrial Fibrillation to Atrial Flutter
- Resolution of atrial fibrillation with induction of general anesthesia: A case report
- Atrial Flutter Conversion in Infants and Children Using Transesophageal Atrial Pacing
- Atrial Fibrillation Developed after Induction of General Anesthesia in an Elderly Patient: A case report
- A case of fetal atrial flutter with hydrops fetalis
