MR Imaging Findings of Lower Extremity Sepsis Caused by Vibrio Vulnificus: A Report of Three Cases
- Affiliations
-
- 1Department of Radiology, Hallym University College of Medicine, Hallym University Sacred Heart Hospital, Anyang, Korea. jnsunghye@hallym.or.kr
- 2Department of Pathology, Hallym University College of Medicine, Hallym University Sacred Heart Hospital, Anyang, Korea.
- 3Department of Internal Medicine, Hallym University College of Medicine, Hallym University Sacred Heart Hospital, Anyang, Korea.
- KMID: 2365052
- DOI: http://doi.org/10.3348/jksr.2017.76.1.54
Abstract
- Lower extremity infection caused by Vibrio vulnificus sepsis is a rapidly progressing fatal condition. Prompt diagnosis followed by early and aggressive treatment with antibiotics and fasciotomy is crucial. In this report, we described lower extremity magnetic resonance (MR) images of three patients with Vibrio vulnificus sepsis. In our cases, MR imaging of lower extremity with Vibrio vulnificus sepsis showed three common findings. First, the MR signal abnormalities appeared simultaneously in all layers, including skin, subcutaneous fat, muscles, and deep fasciae. Second, the inflammation showed symmetry on both legs. Third, none of our cases was accompanied by abscess formation. These imaging features may represent rapid progression of Vibrio vulnificus sepsis and could be helpful for accurate diagnosis, and prompt and aggressive treatment.
MeSH Terms
Figure
-
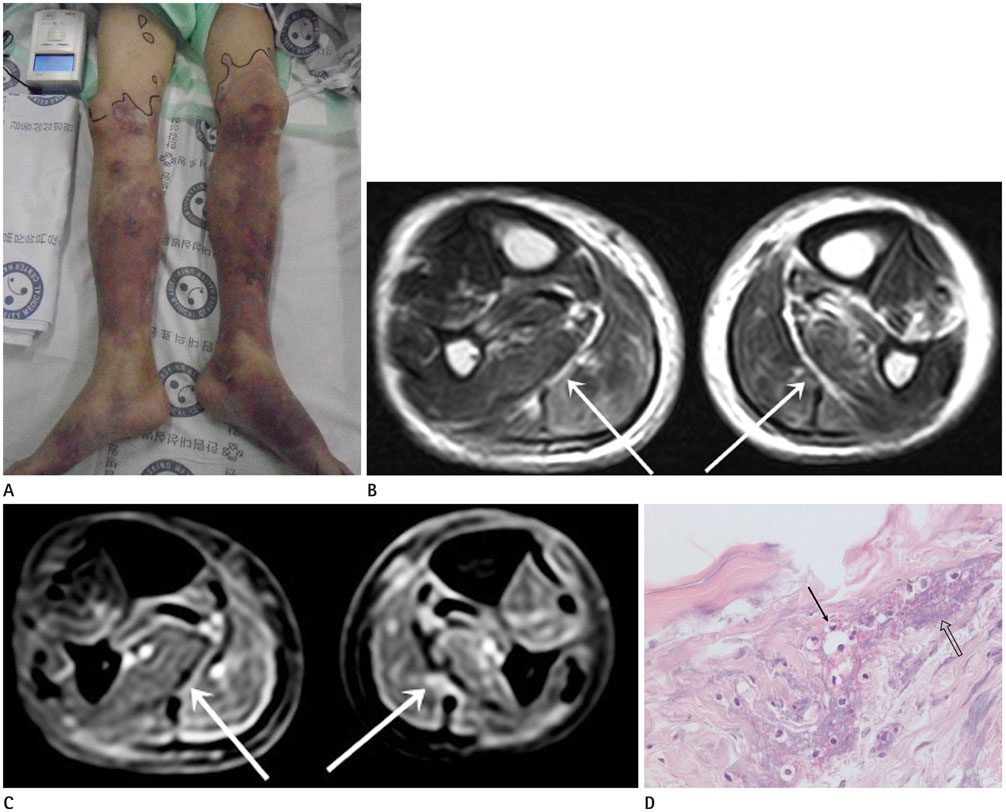
Fig. 1 A 61-year-old man diagnosed as Vibrio vulnificus sepsis (case 1). A. Photograph of bilateral lower extremities demonstrates multifocal erythematous patches, ecchymoses, and cyanotic skin lesions. The upper boundary of the lesion is marked, to determine superior spread of the lesion. B, C. Axial T2-weighted image (B) shows abnormal increased signal intensity in skin, subcutaneous fat, multiple muscles of all compartments, and transverse intermuscular septa (arrows) of both legs. Gadolinum enhanced fat-suppressed T1-weighted image (C) shows enhancement of superficial fascia and transverse intermuscular septa (arrows). There is no abscess in both lower extremities. D. Histologic image of fascial layer of the leg reveals degeneration of fibrous tissue (open arrow) and multifocal neutrophil infiltrations (arrow) (hematoxylin and eosin stain, × 400).
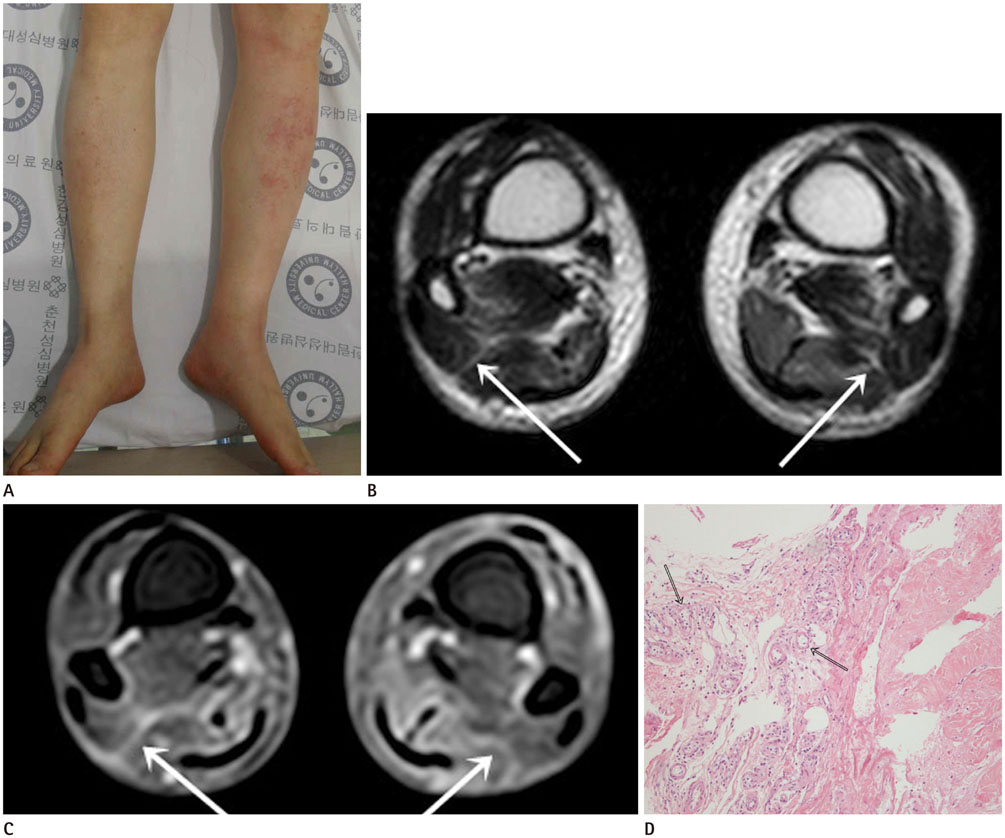
Fig. 2 A 51-year-old man diagnosed as Vibrio vulnificus sepsis (case 2). A. Photograph of bilateral lower extremities shows multiple petechiae and patches. B, C. Axial T2-weighted image (B) shows multifocal patchy high signal intensity in multiple muscles, intermuscular septa (arrows), and overlying subcutaneous fat and skin of both legs. Gadolinum enhanced fat-suppressed T1-weighted image (C) demonstrates thin enhancement along the transverse and posterior intermuscular septa (arrows). There is no abscess in both lower extremities. D. Histologic image of fascia of the leg reveals vascular congestion in the fascia with perivascular neutrophil infiltrations (open arrows) (hematoxylin and eosin stain, × 100).
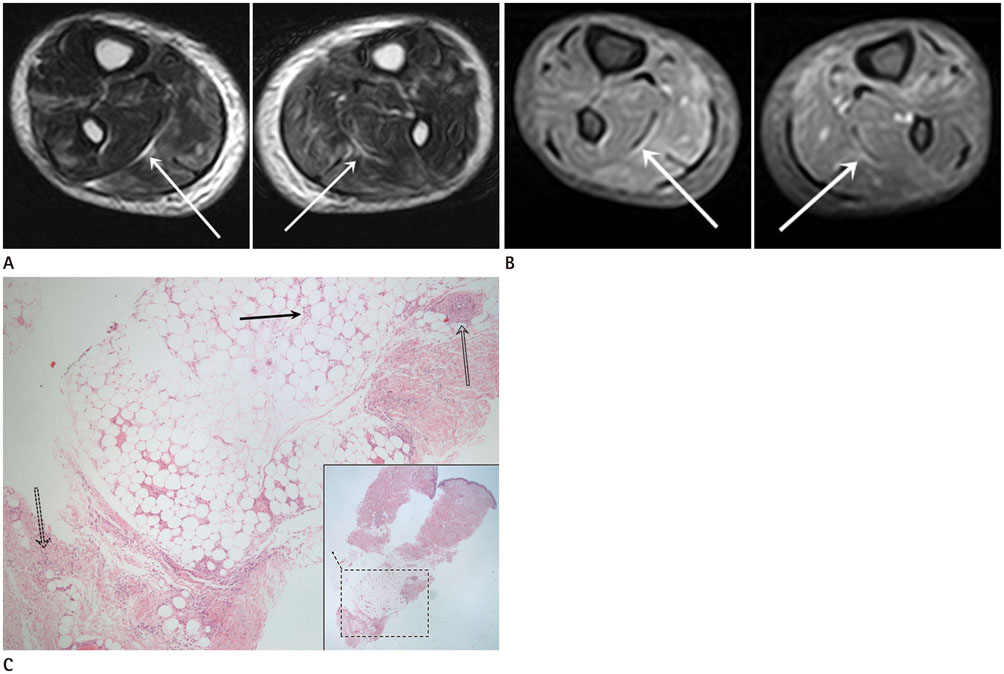
Fig. 3 A 49-year-old man diagnosed as Vibrio vulnificus sepsis (case 3). A, B. Axial T2-weighted MR image (A) shows high signal intensity affecting skin, subcutaneous fat, and multiple muscles, and intermuscular septa (arrows) of both legs. Gadolinum enhanced fat-suppressed T1-weighted image (B) shows mild enhancement of bilateral transverse intermuscular septa (arrows). There is no abscess in both lower extremities. C. Histologic specimen of punch biopsy of the skin lesion in the leg reveals diffusely scattered neutrophils in subcutaneous fat layer (arrow), superficial fascia (dashed arrow), and vascular wall of deep dermis (open arrow) (hematoxylin and eosin stain, × 40). Square box at right below shows histologic specimen (× 12 magnification).
Reference
-
1. Park SD, Shon HS, Joh NJ. Vibrio vulnificus septicemia in Korea: clinical and epidemiologic findings in seventy patients. J Am Acad Dermatol. 1991; 24:397–403.2. Turecki MB, Taljanovic MS, Stubbs AY, Graham AR, Holden DA, Hunter TB, et al. Imaging of musculoskeletal soft tissue infections. Skeletal Radiol. 2010; 39:957–971.3. Paz Maya S, Dualde Beltrán D, Lemercier P, Leiva-Salinas C. Necrotizing fasciitis: an urgent diagnosis. Skeletal Radiol. 2014; 43:577–589.4. Chiang SR, Chuang YC. Vibrio vulnificus infection: clinical manifestations, pathogenesis, and antimicrobial therapy. J Microbiol Immunol Infect. 2003; 36:81–88.5. Haq SM, Dayal HH. Chronic liver disease and consumption of raw oysters: a potentially lethal combination--a review of Vibrio vulnificus septicemia. Am J Gastroenterol. 2005; 100:1195–1199.6. Strom MS, Paranjpye RN. Epidemiology and pathogenesis of Vibrio vulnificus. Microbes Infect. 2000; 2:177–188.7. Horseman MA, Surani S. A comprehensive review of Vibrio vulnificus: an important cause of severe sepsis and skin and soft-tissue infection. Int J Infect Dis. 2011; 15:e157–e166.8. Chaudhry AA, Baker KS, Gould ES, Gupta R. Necrotizing fasciitis and its mimics: what radiologists need to know. AJR Am J Roentgenol. 2015; 204:128–139.9. Kim KT, Kim YJ, Won Lee J, Kim YJ, Park SW, Lim MK, et al. Can necrotizing infectious fasciitis be differentiated from nonnecrotizing infectious fasciitis with MR imaging? Radiology. 2011; 259:816–824.10. Lee JH, Na JB. MR findings of infectious myositis caused by vibrio vulnificus: case report. J Korean Radiol Soc. 2003; 48:285–288.
