Gelatin Sponge Particle Embolization of Spontaneously Ruptured Intrahepatic Arterial Aneurysms in a Patient with Polyarteritis Nodosa: A Case Report
- Affiliations
-
- 1Department of Radiology, Presbyterian Medical Center, Jeonju, Korea. chickh@nate.com
- KMID: 2365048
- DOI: http://doi.org/10.3348/jksr.2017.76.1.25
Abstract
- Multiple intrahepatic arterial aneurysms and spontaneous aneurysmal rupture associated with polyarteritis nodosa leading to hemoperitoneum are extremely rare occurrences, but the conditions can be life-threatening if left untreated because of the risk of massive hemorrhage. We report a case of a high-risk surgical patient with polyarteritis nodosa complicated by spontaneous rupture of multiple intrahepatic arterial aneurysms. He was initially treated with emergency gelatin sponge particle embolization, followed by maintenance steroid treatment. Complete resolution of intrahepatic arterial aneurysms was observed at follow-up.
MeSH Terms
Figure
-
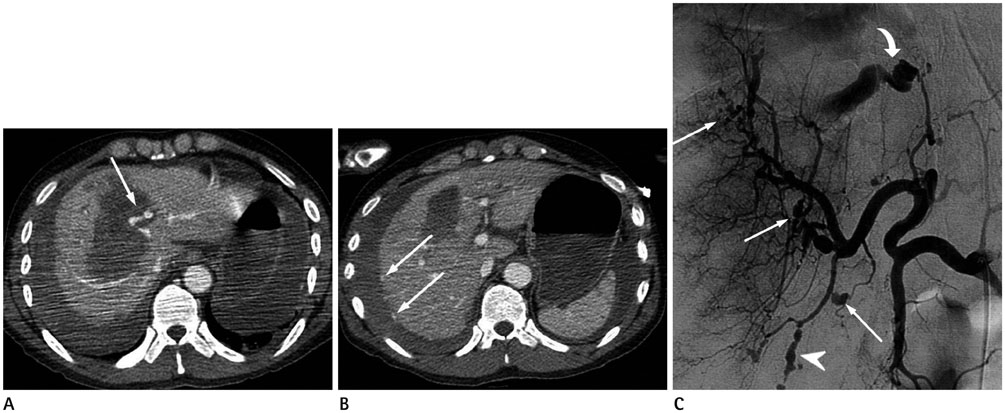
Fig. 1 Spontaneously ruptured intrahepatic arterial aneurysms in a 32-year-old man with polyarteritis nodosa who presented with a sudden-onset epigastric pain. A. Axial contrast-enhanced CT shows an intrahepatic hematoma measuring approximately 10 cm in diameter in segment IV and extravasation of the contrast (arrow). B. Multifocal small contrast extravasations (arrows) on the surface of the liver, and a subcapsular hematoma exceeding 3 cm in thickness with a large amount of hemoperitoneum are seen. C. A selective common hepatic angiogram shows multiple aneurysms of varying sizes (arrows) with multifocal vascular ectasia and stenoses (arrowhead). Note the active extravasation of the contrast from the ruptured left medial hepatic artery (curved arrow), presumed to be extravasation of the contrast observed in segment IV on the CT scan.
Reference
-
1. Lightfoot RW Jr, Michel BA, Bloch DA, Hunder GG, Zvaifler NJ, McShane DJ, et al. The American College of Rheumatology 1990 criteria for the classification of polyarteritis nodosa. Arthritis Rheum. 1990; 33:1088–1093.2. Parangi S, Oz MC, Blume RS, Bixon R, Laffey KJ, Perzin KH, et al. Hepatobiliary complications of polyarteritis nodosa. Arch Surg. 1991; 126:909–912.3. Stanson AW, Friese JL, Johnson CM, McKusick MA, Breen JF, Sabater EA, et al. Polyarteritis nodosa: spectrum of angiographic findings. Radiographics. 2001; 21:151–159.4. Parent BA, Cho SW, Buck DG, Nalesnik MA, Gamblin TC. Spontaneous rupture of hepatic artery aneurysm associated with polyarteritis nodosa. Am Surg. 2010; 76:1416–1419.5. Leung VK, Lam CY, Chan CC, Ng WL, Loke TK, Luk IS, et al. Spontaneous intra-hepatic haemorrhage in a patient with fever of unknown origin. Hong Kong Med J. 2007; 13:319–322.6. Hagspiel KD, Angle JF, Spinosa DJ, Matsumoto AH. Diagnosis please. Case 13: polyarteritis nodosa--systemic necrotizing vasculitis with involvement of hepatic and superior mesenteric arteries. Radiology. 1999; 212:359–364.7. Rhodes ES, Pekala JS, Gemery JM, Dickey KW. Case 129: polyarteritis nodosa. Radiology. 2008; 246:322–326.8. Darras-Joly C, Lortholary O, Cohen P, Brauner M, Guillevin L. Regressing microaneurysms in 5 cases of hepatitis B virus related polyarteritis nodosa. J Rheumatol. 1995; 22:876–880.9. Bauer JR, Ray CE. Transcatheter arterial embolization in the trauma patient: a review. Semin Intervent Radiol. 2004; 21:11–22.10. Korean Society of Interventional Radiology. Interventional radiology. 2nd ed. Seoul: Ilchokak;2014. p. 368–370.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Hybrid Surgery to Treat Multiple Visceral Aneurysms Secondary to Polyarteritis Nodosa
- Hemobilia from Ruptured Hepatic Artery Aneurysm in Polyarteritis Nodosa
- A Case of Spontaneous Repture of Renal Artery Aneurysm in Polyarteritis Nodosa
- Polyarteritis Nodosa Complicated by Chronic Total Occlusion Accompanying Aneurysms on All Coronary Arteries
- Ischemic Pseudomembranous Colitis with Perforation due to Polyarteritis Nodosa
