Fucntional and Radiological Outcome of Surgical Management of Acetabular Fractures in Tertiary Care Hospital
- Affiliations
-
- 1Department of Orthopedic Surgery, Liaquat National Hospital, Karachi, Pakistan. drfaizi1@yahoo.com
- KMID: 2364699
- DOI: http://doi.org/10.5371/hp.2016.28.4.217
Abstract
- PURPOSE
Acetabular fractures are mainly caused by trauma and the incidence is rising in developing countries. Initially these fractures were managed conservatively, due to lack of specialized and dedicated acetabulum surgery centres. Our aim is to study the radiological and functional outcomes of surgical management of acetabular fractures in tertiary care hospital.
MATERIALS AND METHODS
Total 50 patients were enrolled. The patients with acetabular fractures were enrolled between the years 2012 to 2014. Patients were evaluated clinically with Harris hip score (HHS) and radiologically with Matta outcome grading. The factors examined include age, gender, fracture pattern, time between injury and surgery, initial displacement and quality of reduction on the final outcome.
RESULTS
There were 34 males and 16 females. Mean age was 44.20±11.65 years while mean duration of stay was 9.28±2.36 days. Duration of follow-up was 24 months. Most common mechanism of injury was motor vehicle accident (n=37, 74.0%). Open reduction and internal fixation of fractures were performed using reconstruction plates. Mean HHS at 24 months was 82.36±8.55. The clinical outcome was acceptable (excellent or good) in 35 (70.0%) cases and not acceptable (fair or poor) in 15 (30.0%) cases. The radiological outcome was anatomical in 39 (78.0%) cases, congruent in 5 (10.0%) cases, incongruent in 6 (12.0%) cases.
CONCLUSION
Study results indicated that mechanism of injury, time between injury and surgery, initial degree of displacement and quality of reduction had significant effect on functional as well as radiological outcome.
MeSH Terms
Figure
-

Fig. 1 X-ray pelvis (anteroposterior view) of skeletally mature 48 year-old male patient showing transverse fracture with inward subluxation of left hip.
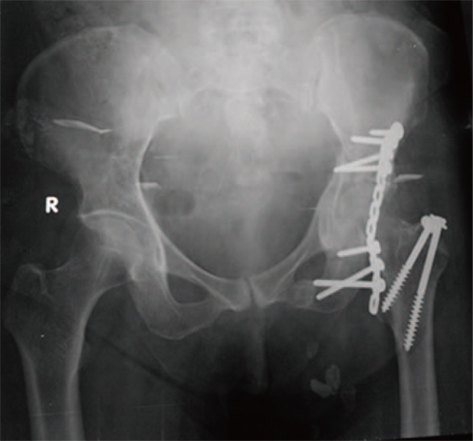
Fig. 2 X-ray pelvis (anteroposterior view) of same patient taken on first postoperative day showing open reduction and internal fixation of left hip with reconstruction plate. Trochanteric osteotomy was performed for better visualization of fracture site and was closed by two cannulated screws.
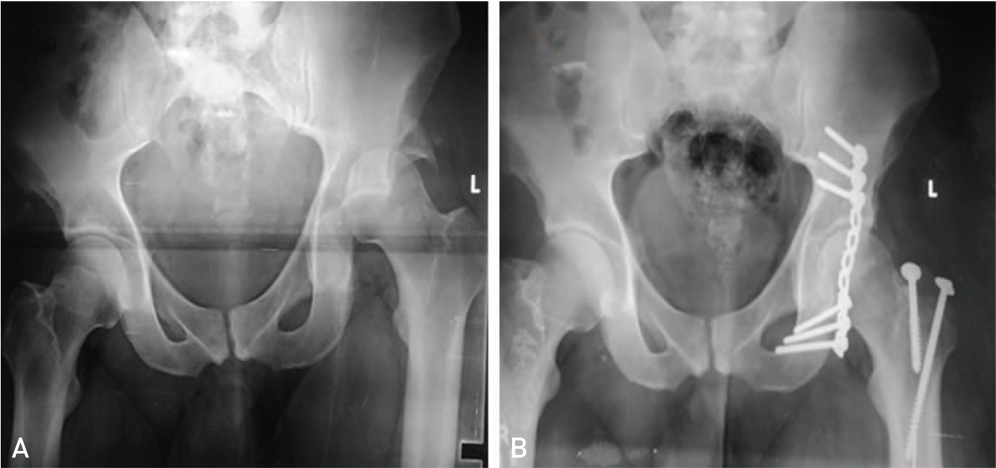
Fig. 3 (A) X-ray pelvis (anteroposterior view) of skeletally mature 32 year old male patient showing fracture of posterior wall of left acetabulum. (B) X-ray pelvis (anteroposterior view) of same patient showing open reduction and internal fixation with reconstruction plate. Trochancteric osteotomy was performed for better visualisation of fracture site which was closed by two cannulated screws.
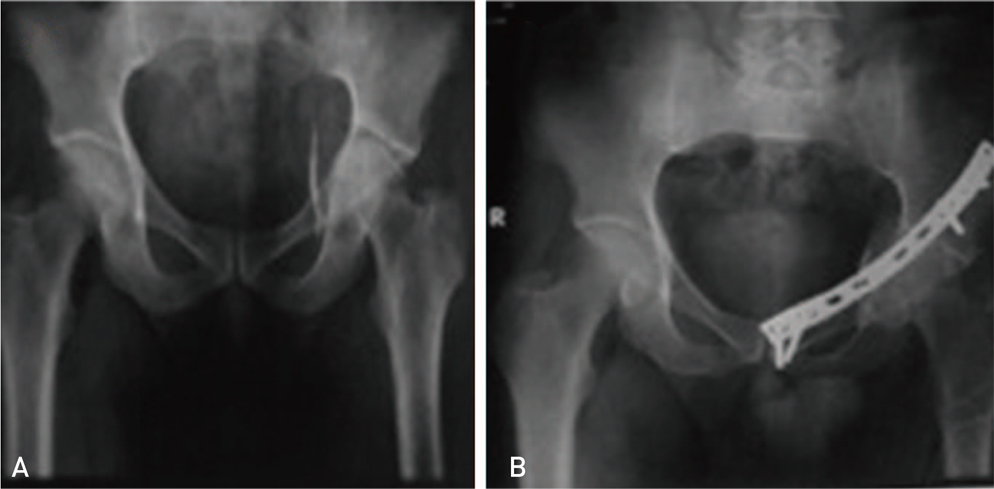
Fig. 4 (A) X-ray pelvis (anteroposterior view) of skeletally mature 50 year old male patient showing 10 days old displaced anterior column and medial wall fracture. (B) X-ray pelvis (anteroposterior view) of same patient showing open reduction and internal fixation with inward subluxation of left hip and poor restoration of five anatomical lines.
Reference
-
1. Rao VS, Chandrasekhar P, Rao AL, Rao VB. Results of surgically treated displaced acetabular fractures among adults. Clin Proc NIMS. 2008; 17:2.2. Ghaffar A, Hyder AA, Masud TI. The burden of road traffic injuries in developing countries: the 1st national injury survey of Pakistan. Public Health. 2004; 118:211–217.
Article3. Khan SH, Ara I, Raza S, Sipra S. Functional outcome of surgery in patients with acetabular fractures. J Ayub Med Coll Abbottabad. 2013; 25:60–63.4. Pohlemann T, Gänsslen A, Stief CH. Complex injuries of the pelvis and acetabulum. Orthopade. 1998; 27:32–44.5. Glas PY, Fessy MH, Carret JP, Béjui-Hugues J. Surgical treatment of acetabular fractures: outcome in a series of 60 consecutive cases. Rev Chir Orthop Reparatrice Appar Mot. 2001; 87:529–538.6. Giannoudis PV, Bircher M, Pohlemann T. Advances in pelvic and acetabular surgery. Injury. 2007; 38:395–396.
Article7. Letournel E. Acetabulum fractures: classification and management. Clin Orthop Relat Res. 1980; (151):81–106.
Article8. Judet R, Judet J, Letournel E. Fractures of the acetabulum: classification and surgical approaches for open reduction. Preliminary report. J Bone Joint Surg Am. 1964; 46:1615–1646.9. Matta JM. Fractures of the acetabulum: accuracy of reduction and clinical results in patients managed operatively within three weeks after the injury. J Bone Joint Surg Am. 1996; 78:1632–1645.10. Matta JM, Mehne DK, Roffi R. Fractures of the acetabulum. Early results of a prospective study. Clin Orthop Relat Res. 1986; (205):241–250.11. Shrestha D, Dhoju D, Shrestha R, Sharma V. Acetabular fracture: Retrospective analysis of thirty three consecutive cases with operative management. Kathmandu Univ Med J (KUMJ). 2014; 12:279–287.
Article12. Gupta RK, Singh H, Dev B, Kansay R, Gupta P, Garg S. Results of operative treatment of acetabular fractures from the Third World--how local factors affect the outcome. Int Orthop. 2009; 33:347–352.
Article13. Magu NK, Rohilla R, Arora S. Conservatively treated acetabular fractures: A retrospective analysis. Indian J Orthop. 2012; 46:36–45.
Article14. Marchetti P, Binazzi R, Vaccari V, et al. Long-term results with cementless Fitek (or Fitmore) cups. J Arthroplasty. 2005; 20:730–737.
Article15. Acetabulum fractures [Internet]. New York: Medscape;2016 Aug 8. cited 2016 May 2. Available from: http://emedicine.medscape.com/article/1246057-overview#a9.16. Kim HT, Ahn JM, Hur JO, Lee JS, Cheon SJ. Reconstruction of acetabular posterior wall fractures. Clin Orthop Surg. 2011; 3:114–120.
Article17. Lehmann W, Hoffmann M, Fensky F, et al. What is the frequency of nerve injuries associated with acetabular fractures? Clin Orthop Relat Res. 2014; 472:3395–3403.
Article18. Suzuki T, Morgan SJ, Smith WR, Stahel PF, Gillani SA, Hak DJ. Postoperative surgical site infection following acetabular fracture fixation. Injury. 2010; 41:396–399.
Article19. Meena UK, Tripathy SK, Sen RK, Aggarwal S, Behera P. Predictors of postoperative outcome for acetabular fractures. Orthop Traumatol Surg Res. 2013; 99:929–935.
Article20. O'Toole RV, Hui E, Chandra A, Nascone JW. How often does open reduction and internal fixation of geriatric acetabular fractures lead to hip arthroplasty? J Orthop Trauma. 2014; 28:148–153.21. Hussain KSA, Kancherla NR, Kanugula SK, Patnala C. Analysis of displaced acetabular fractures in adults treated with open reduction and internal fixation. Int J Res Orthop. 2016; 2:99–103.
Article22. Moed BR, Yu PH, Gruson KI. Functional outcomes of acetabular fractures. J Bone Joint Surg Am. 2003; 85-A:1879–1883.
Article23. Kreder HJ, Rozen N, Borkhoff CM, et al. Determinants of functional outcome after simple and complex acetabular fractures involving the posterior wall. J Bone Joint Surg Br. 2006; 88:776–782.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Outcomes of Surgical Treatment of Acetabular Fractures with a Minimum of 1-Year Follow-up
- Surgical Treatment of Displaced Acetabular Fractures - focused on Complications after open reduction -
- Clinical Results of Surgical Treatment of Acetabular Fractures according to Quality of Reduction
- The Surgical Treatment of displaced Acetabular Fracture
- Anterior Approach for the Acetabular Fractures
