Robotic thyroidectomy: Evolution and Outcomes
- Affiliations
-
- 1Department of Otolaryngology-Head and Neck Surgery, College of Medicine, Hanyang University, Seoul, Korea. kytae@hanyang.ac.kr
- KMID: 2361193
- DOI: http://doi.org/10.7599/hmr.2016.36.4.205
Abstract
- Recently robotic thyroidectomy has gained its popularity for the treatment of differentiated thyroid cancer and benign thyroid tumors. It has been developed to overcome the drawbacks of conventional open trans-cervical thyroidectomy, which is an apparent neck wound that is visible unless concealed with clothes. Robotic thyroidectomy provides surgeons with three-dimensional magnified view and multiarticulated robotic arms that can stabilize hand tremors. It also has advantages over conventional trans-cervical thyroidectomy that include recovery of voice symptoms and acoustic parameters along with superior cosmetic outcomes. Robotic thyroidectomy results in equivalent surgical outcomes including oncologic safety and complications compared with conventional thyroidectomy. Various approaches including transaxillary, postauricular facelift, and breast-axillary approaches have been developed for robotic thyroidectomy. Recently, the indication of robotic surgery has been extended to neck dissection of the lateral compartment. Herein we summarize the indication, procedures, and efficacy of robotic thyroidectomy, and also introduce our experience with robotic thyroidectomy.
MeSH Terms
Figure
-
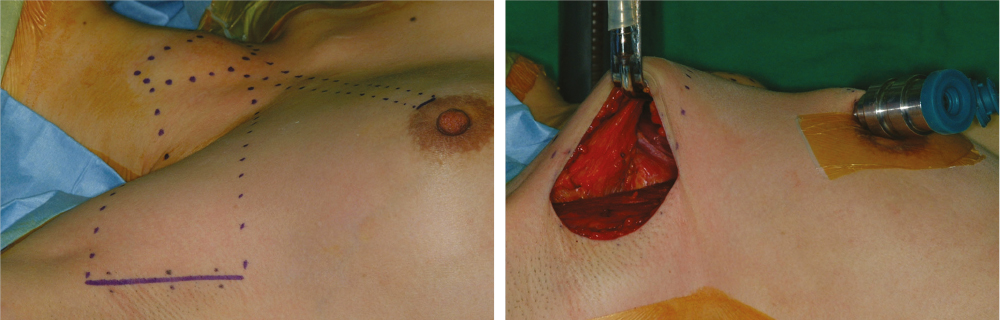
Fig. 1 Gasless unilateral axillo-breast approach (right side approach). (A) Incisions consist of a main vertical axillary incision and a minor incision in the circum-areolar margin. (B) After flap dissection, a retractor is inserted in the main axillary space, and a trocar for Prograsp forceps is inserted in the minor incision site.
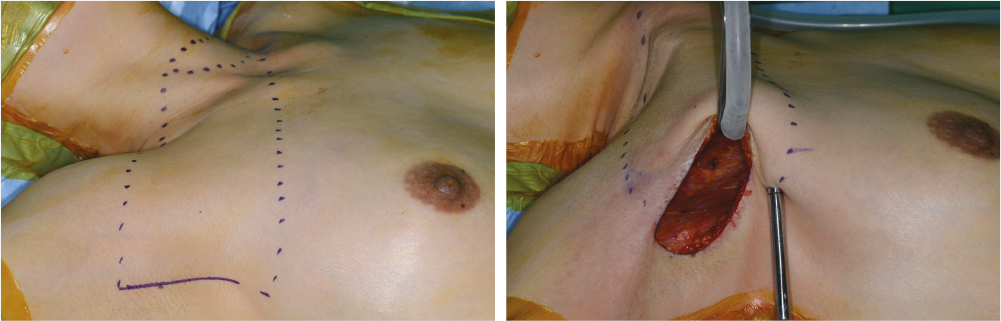
Fig. 2 Gasless unilateral axillary approach (right side approach). (A) A main vertical incision is made in the axillary fossa, and a minor incision is made inferior to the main incision. (B) After the flap is dissected, the retractor is inserted in the main axillary incision, and a trocar for Harmonic curved shears is inserted in the accessory incision site.
Cited by 2 articles
-
Review of Computer-Aided Surgery
Byung-Ju Yi
Hanyang Med Rev. 2016;36(4):203-204. doi: 10.7599/hmr.2016.36.4.203.Transoral Robotic Thyroidectomy: Description of the Surgical Technique in the Cadaveric Model
Özer Makay, Varlık Erol
J Endocr Surg. 2018;18(2):155-160. doi: 10.16956/jes.2018.18.2.155.
Reference
-
1. Han MA, Choi KS, Lee HY, Kim Y, Jun JK, Park EC. Current status of thyroid cancer screening in Korea: results from a nationwide interview survey. Asian Pac J Cancer Prev. 2011; 12:1657–1663.2. Palme CE, Waseem Z, Raza SN, Eski S, Walfish P, Freeman JL. Management and outcome of recurrent well-differentiated thyroid carcinoma. Arch Otolaryngol Head Neck Surg. 2004; 130:819–824.
Article3. Al-Sarraf M. Treatment of locally advanced head and neck cancer: historical and critical review. Cancer Control. 2002; 9:387–399.
Article4. Tae K, Ji YB, Cho SH, Lee SH, Kim DS, Kim TW. Early surgical outcomes of robotic thyroidectomy by a gasless unilateral axillo-breast or axillary approach for papillary thyroid carcinoma: 2 years' experience. Head Neck. 2012; 34:617–625.
Article5. Huscher CS, Chiodini S, Napolitano C, Recher A. Endoscopic right thyroid lobectomy. Surg Endosc. 1997; 11:877.
Article6. Miccoli P, Berti P, Conte M, Bendinelli C, Marcocci C. Minimally invasive surgery for thyroid small nodules: preliminary report. J Endocrinol Invest. 1999; 22:849–851.
Article7. Duncan TD, Rashid Q, Speights F, Ejeh I. Endoscopic transaxillary approach to the thyroid gland: our early experience. Surg Endosc. 2007; 21:2166–2171.
Article8. Choe JH, Kim SW, Chung KW, Park KS, Han W, Noh DY, et al. Endoscopic thyroidectomy using a new bilateral axillo-breast approach. World J Surg. 2007; 31:601–606.
Article9. Sun GH, Peress L, Pynnonen MA. Systematic review and meta-analysis of robotic vs conventional thyroidectomy approaches for thyroid disease. Otolaryngol Head Neck Surg. 2014; 150:520–532.
Article10. Goh HK, Ng YH, Teo DT. Minimally invasive surgery for head and neck cancer. Lancet Oncol. 2010; 11:281–286.
Article11. Lobe TE, Wright SK, Irish MS. Novel uses of surgical robotics in head and neck surgery. J Laparoendosc Adv Surg Tech A. 2005; 15:647–652.
Article12. Tanna N, Joshi AS, Glade RS, Zalkind D, Sadeghi N. Da Vinci robot-assisted endocrine surgery: novel applications in otolaryngology. Otolaryngol Head Neck Surg. 2006; 135:633–635.
Article13. Kang SW, Jeong JJ, Yun JS, Sung TY, Lee SC, Lee YS, et al. Robot-assisted endoscopic surgery for thyroid cancer: experience with the first 100 patients. Surg Endosc. 2009; 23:2399–2406.
Article14. Tae K, Ji YB, Jeong JH, Lee SH, Jeong MA, Park CW. Robotic thyroidectomy by a gasless unilateral axillo-breast or axillary approach: our early experiences. Surg Endosc. 2011; 25:221–228.
Article15. Tae K, Ji YB, Cho SH, Kim KR, Kim DW, Kim DS. Initial experience with a gasless unilateral axillo-breast or axillary approach endoscopic thyroidectomy for papillary thyroid microcarcinoma: comparison with conventional open thyroidectomy. Surg Laparosc Endosc Percutan Tech. 2011; 21:162–169.
Article16. Ikeda Y, Takami H, Sasaki Y, Kan S, Niimi M. Endoscopic resection of thyroid tumors by the axillary approach. J Cardiovasc Surg (Torino). 2000; 41:791–792.17. Lee J, Chung WY. Robotic thyroidectomy and neck dissection: past, present, and future. Cancer J. 2013; 19:151–161.18. Song CM, Ji YB, Bang HS, Park CW, Kim H, Tae K. Long-term sensory disturbance and discomfort after robotic thyroidectomy. World J Surg. 2014; 38:1743–1748.
Article19. Song CM, Cho YH, Ji YB, Jeong JH, Kim DS, Tae K. Comparison of a gasless unilateral axillo-breast and axillary approach in robotic thyroidectomy. Surg Endosc. 2013; 27:3769–3775.
Article20. Sung ES, Ji YB, Song CM, Yun BR, Chung WS, Tae K. Robotic Thyroidectomy: Comparison of a Postauricular Facelift Approach with a Gasless Unilateral Axillary Approach. Otolaryngol Head Neck Surg. 2016; 154:997–1004.21. Singer MC, Seybt MW, Terris DJ. Robotic facelift thyroidectomy: I. Preclinical simulation and morphometric assessment. Laryngoscope. 2011; 121:1631–1635.
Article22. Terris DJ, Singer MC, Seybt MW. Robotic facelift thyroidectomy: II. Clinical feasibility and safety. Laryngoscope. 2011; 121:1636–1641.
Article23. Terris DJ, Singer MC, Seybt MW. Robotic facelift thyroidectomy: patient selection and technical considerations. Surg Laparosc Endosc Percutan Tech. 2011; 21:237–242.24. Song CM, Jung YH, Sung MW, Kim KH. Endoscopic resection of the submandibular gland via a hairline incision: a new surgical approach. Laryngoscope. 2010; 120:970–974.
Article25. Grover N, D'Souza A. Facelift approach for parotidectomy: an evolving aesthetic technique. Otolaryngol Head Neck Surg. 2013; 148:548–556.26. Song CM, Ji YB, Kim KR, Tae K. Robot-assisted excision of branchial cleft cysts using a postauricular facelift approach. Auris Nasus Larynx. 2015; 42:424–427.
Article27. Terris DJ, Singer MC. Qualitative and quantitative differences between 2 robotic thyroidectomy techniques. Otolaryngol Head Neck Surg. 2012; 147:20–25.
Article28. Berber E, Bernet V, Fahey TJ 3rd, Kebebew E, Shaha A, Stack BC Jr, et al. American Thyroid Association Statement on Remote-Access Thyroid Surgery. Thyroid. 2016; 26:331–337.
Article29. Shimazu K, Shiba E, Tamaki Y, Takiguchi S, Taniguchi E, Ohashi S, et al. Endoscopic thyroid surgery through the axillo-bilateral-breast approach. Surg Laparosc Endosc Percutan Tech. 2003; 13:196–201.
Article30. Tae K, Song CM, Ji YB, Sung ES, Jeong JH, Kim DS. Oncologic outcomes of robotic thyroidectomy: 5-year experience with propensity score matching. Surg Endosc. 2016.
Article31. Lee J, Nah KY, Kim RM, Ahn YH, Soh EY, Chung WY. Differences in postoperative outcomes, function, and cosmesis: open versus robotic thyroidectomy. Surg Endosc. 2010; 24:3186–3194.
Article32. Lee J, Yun JH, Nam KH, Soh EY, Chung WY. The learning curve for robotic thyroidectomy: a multicenter study. Ann Surg Oncol. 2011; 18:226–232.
Article33. Lee J, Lee JH, Nah KY, Soh EY, Chung WY. Comparison of endoscopic and robotic thyroidectomy. Ann Surg Oncol. 2011; 18:1439–1446.
Article34. Tae K, Song CM, Ji YB, Kim KR, Kim JY, Choi YY. Comparison of surgical completeness between robotic total thyroidectomy versus open thyroidectomy. Laryngoscope. 2014; 124:1042–1047.
Article35. Jackson NR, Yao L, Tufano RP, Kandil EH. Safety of robotic thyroidectomy approaches: meta-analysis and systematic review. Head Neck. 2014; 36:137–143.
Article36. Landry CS, Grubbs EG, Morris GS, Turner NS, Holsinger FC, Lee JE, et al. Robot assisted transaxillary surgery (RATS) for the removal of thyroid and parathyroid glands. Surgery. 2011; 149:549–555.
Article37. Kuppersmith RB, Holsinger FC. Robotic thyroid surgery: an initial experience with North American patients. Laryngoscope. 2011; 121:521–526.
Article38. Song CM, Ji YB, Bang HS, Park CW, Kim DS, Tae K. Quality of life after robotic thyroidectomy by a gasless unilateral axillary approach. Ann Surg Oncol. 2014; 21:4188–4194.
Article39. Ji YB, Song CM, Bang HS, Lee SH, Park YS, Tae K. Long-term cosmetic outcomes after robotic/endoscopic thyroidectomy by a gasless unilateral axillo-breast or axillary approach. J Laparoendosc Adv Surg Tech A. 2014; 24:248–253.
Article40. Song CM, Yun BR, Ji YB, Sung ES, Kim KR, Tae K. Long-Term Voice Outcomes After Robotic Thyroidectomy. World J Surg. 2016; 40:110–116.
Article41. Tae K, Kim KY, Yun BR, Ji YB, Park CW, Kim DS, et al. Functional voice and swallowing outcomes after robotic thyroidectomy by a gasless unilateral axillo-breast approach: comparison with open thyroidectomy. Surg Endosc. 2012; 26:1871–1877.
Article42. Song CM, Ji YB, Bang HS, Kim KR, Kim H, Tae K. Postoperative Pain After Robotic Thyroidectomy by a Gasless Unilateral Axillo-Breast or Axillary Approach. Surg Laparosc Endosc Percutan Tech. 2015; 25:478–482.
Article43. Kang SW, Lee SH, Ryu HR, Lee KY, Jeong JJ, Nam KH, et al. Initial experience with robot-assisted modified radical neck dissection for the management of thyroid carcinoma with lateral neck node metastasis. Surgery. 2010; 148:1214–1221.
Article44. Kim WS, Koh YW, Byeon HK, Park YM, Chung HJ, Kim ES, et al. Robot-assisted neck dissection via a transaxillary and retroauricular approach versus a conventional transcervical approach in papillary thyroid cancer with cervical lymph node metastases. J Laparoendosc Adv Surg Tech A. 2014; 24:367–372.
Article45. Song CM, Ji YB, Sung ES, Kim DS, Koo HR, Tae K. Comparison of Robotic versus Conventional Selective Neck Dissection and Total Thyroidectomy for Papillary Thyroid Carcinoma. Otolaryngol Head Neck Surg. 2016; 154:1005–1013.
Article46. Song CM, Park JS, Park W, Ji YB, Cho SH, Tae K. Feasibility of Charcoal Tattooing for Localization of Metastatic Lymph Nodes in Robotic Selective Neck Dissection for Papillary Thyroid Carcinoma. Ann Surg Oncol. 2015; 22:Suppl 3. S669–S675.
Article47. Mandapathil M, Greene B, Wilhelm T. Transoral surgery using a novel single-port flexible endoscope system. Eur Arch Otorhinolaryngol. 2015; 272:2451–2456.
Article48. Herz D, DaJusta D, Ching C, McLeod D. Segmental arterial mapping during pediatric robot-assisted laparoscopic heminephrectomy: A descriptive series. J Pediatr Urol. 2016; 12:266.e1–266.e6.
Article49. Abboudi H, Khan MS, Aboumarzouk O, Guru KA, Challacombe B, Dasgupta P, et al. Current status of validation for robotic surgery simulators - a systematic review. BJU Int. 2013; 111:194–205.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Robotic Thyroidectomy: Pros and Cons of Various Surgical Approaches
- Robotic and Endoscopic Thyroid Surgery: Evolution and Advances
- Robotic Transoral Thyroidectomy: Right Thyroidectomy and Ipsilateral Central Neck Dissection with da Vinci Si Surgical System
- Transoral Robotic Thyroidectomy: The Overview and Suggestions for Future Research in New Minimally Invasive Thyroid Surgery
- Transoral Robotic Thyroidectomy
