Semi-Circumferential Decompression: Microsurgical Total en-bloc Ligamentum Flavectomy to Treat Lumbar Spinal Stenosis with Grade I Degenerative Spondylolisthesis
- Affiliations
-
- 1Department of Orthopedic Surgery, Bundang Jesaeng General Hospital, Daejin Medical Center, Seongnam, Korea. yslee2808@gmail.com
- KMID: 2360261
- DOI: http://doi.org/10.4055/cios.2015.7.4.470
Abstract
- BACKGROUND
To describe and assess clinical outcomes of the semi-circumferential decompression technique for microsurgical en-bloc total ligamentum flavectomy with preservation of the facet joint to treat the patients who have a lumbar spinal stenosis with degenerative spondylolisthesis.
METHODS
We retrospectively analyzed the clinical and radiologic outcomes of 19 patients who have a spinal stenosis with Meyerding grade I degenerative spondylolisthesis. They were treated using the "semi-circumferential decompression" method. We evaluated improvements in back and radiating pain using a visual analogue scale (VAS) and the Oswestry Disability Index (ODI). We also evaluated occurrence of spinal instability on radiological exam using percentage slip and slip angle.
RESULTS
The mean VAS score for back pain decreased significantly from 6.3 to 4.3, although some patients had residual back pain. The mean VAS for radiating pain decreased significantly from 8.3 to 2.5. The ODI score improved significantly from 25.3 preoperatively to 10.8 postoperatively. No significant change in percentage slip was observed (10% preoperatively vs. 12.2% at the last follow-up). The dynamic percentage slip (gap in percentage slip between flexion and extension X-ray exams) did not change significantly (5.2% vs. 5.8%). Slip angle and dynamic slip angle did not change (3.2° and 8.2° vs. 3.6° and 9.2°, respectively).
CONCLUSIONS
The results suggested that semi-circumferential decompression is a clinically recommendable procedure that can improve pain. This procedure does not cause spinal instability when treating patients who have a spinal stenosis with degenerative spondylolisthesis.
Keyword
MeSH Terms
Figure
-
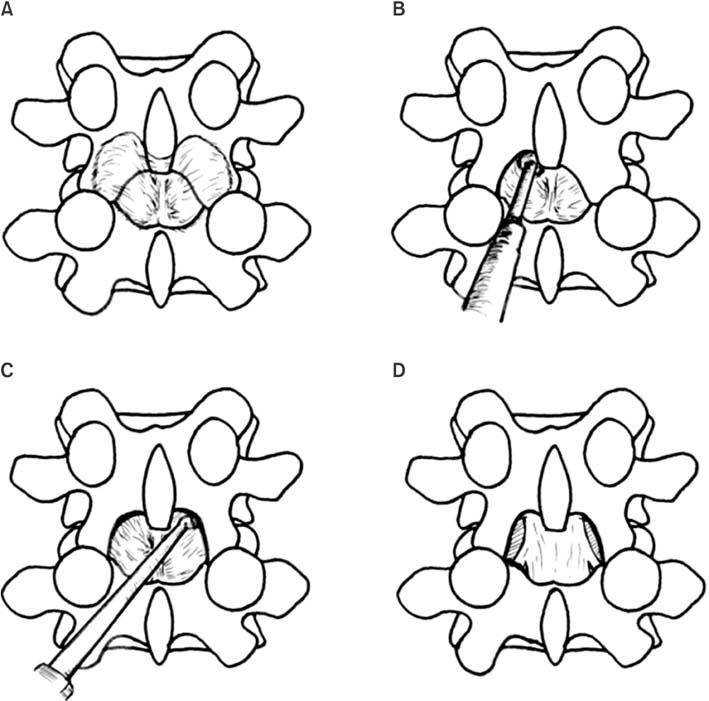
Fig. 1 (A) Preoperative state of ligamentum flavum. (B, C) Ligamentum flavum is detached from the lamina using a currette. (D) After en-bloc ligamentum flavectomy, dura mater is exposed.
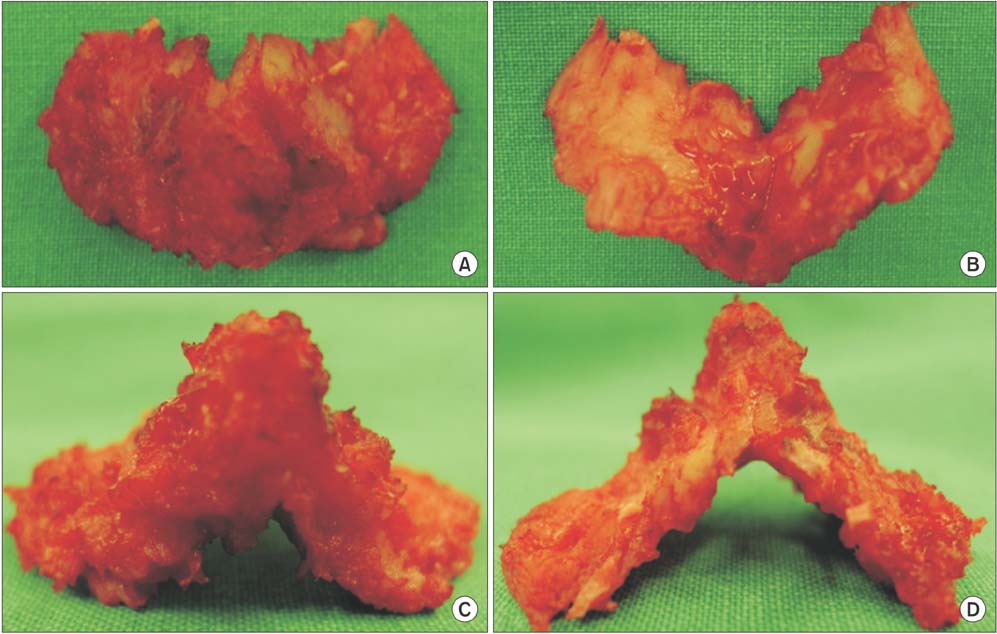
Fig. 2 The ligamentum flavum, which is in the shape of a butterfly, was removed en-bloc. (A) Dorsal surface, (B) ventral surface, (C) distal border, and (D) proximal border.
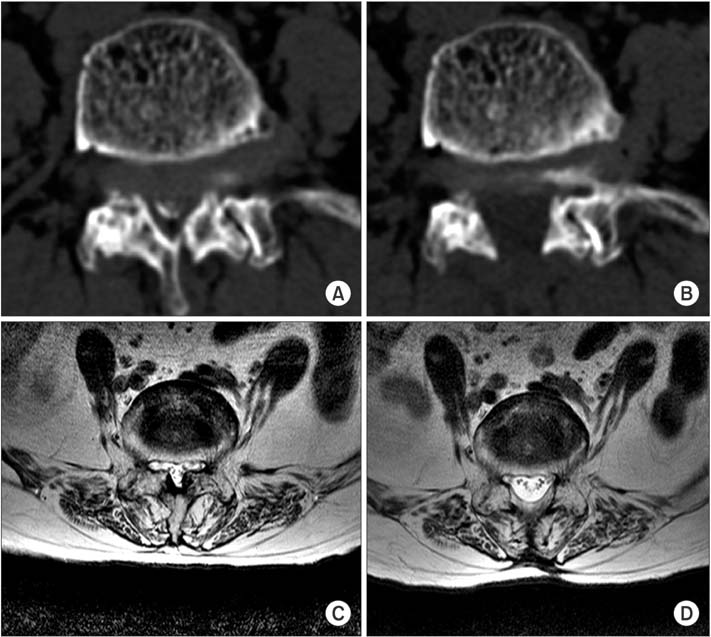
Fig. 3 Preoperative (A, C) and postoperative (B, D) axial computed tomography scans and magnetic resonance images show the facet joint at the spondylolisthesis level in a representative patient who underwent semicircumferential decompression preserving the facet joints. A bilateral laminotomy and total ligamentum flavectomy were performed, and the facet joint was completely preserved.
Reference
-
1. Eismont FJ, Norton RP, Hirsch BP. Surgical management of lumbar degenerative spondylolisthesis. J Am Acad Orthop Surg. 2014; 22(4):203–213.
Article2. Fischgrund JS, Mackay M, Herkowitz HN, Brower R, Montgomery DM, Kurz LT. 1997 Volvo Award winner in clinical studies Degenerative lumbar spondylolisthesis with spinal stenosis: a prospective, randomized study comparing decompressive laminectomy and arthrodesis with and without spinal instrumentation. Spine (Phila Pa 1976). 1997; 22(24):2807–2812.3. Ragab AA, Fye MA, Bohlman HH. Surgery of the lumbar spine for spinal stenosis in 118 patients 70 years of age or older. Spine (Phila Pa 1976). 2003; 28(4):348–353.
Article4. Carreon LY, Puno RM, Dimar JR 2nd, Glassman SD, Johnson JR. Perioperative complications of posterior lumbar decompression and arthrodesis in older adults. J Bone Joint Surg Am. 2003; 85(11):2089–2092.
Article5. Weiner BK, Fraser RD, Peterson M. Spinous process osteotomies to facilitate lumbar decompressive surgery. Spine (Phila Pa 1976). 1999; 24(1):62–66.
Article6. Nakanishi K, Tanaka N, Fujimoto Y, et al. Medium-term clinical results of microsurgical lumbar flavectomy that preserves facet joints in cases of lumbar degenerative spondylolisthesis: comparison of bilateral laminotomy with bilateral decompression by a unilateral approach. J Spinal Disord Tech. 2013; 26(7):351–358.
Article7. Musluman AM, Cansever T, Yilmaz A, Cavusoglu H, Yuce I, Aydın Y. Midterm outcome after a microsurgical unilateral approach for bilateral decompression of lumbar degenerative spondylolisthesis. J Neurosurg Spine. 2012; 16(1):68–76.
Article8. Newman PH, Stone KH. The etiology of spondylolisthesis. J Bone Joint Surg Br. 1963; 45(1):39–59.
Article9. Sengupta DK, Herkowitz HN. Degenerative spondylolisthesis: review of current trends and controversies. Spine (Phila Pa 1976). 2005; 30:6 Suppl. S71–S81.10. Herkowitz HN, Kurz LT. Degenerative lumbar spondylolisthesis with spinal stenosis: a prospective study comparing decompression with decompression and intertransverse process arthrodesis. J Bone Joint Surg Am. 1991; 73(6):802–808.
Article11. Mardjetko SM, Connolly PJ, Shott S. Degenerative lumbar spondylolisthesis: a meta-analysis of literature 1970-1993. Spine (Phila Pa 1976). 1994; 19:20 Suppl. 2256S–2265S.12. Chung NS, Jeon CH. Surgical treatment of degenerative and isthmic spondylolisthesis. J Korean Soc Spine Surg. 2009; 16(3):228–234.
Article13. Kirkaldy-Willis WH, Hill RJ. A more precise diagnosis for low-back pain. Spine (Phila Pa 1976). 1979; 4(2):102–109.
Article14. Matsunaga S, Sakou T, Morizono Y, Masuda A, Demirtas AM. Natural history of degenerative spondylolisthesis: pathogenesis and natural course of the slippage. Spine (Phila Pa 1976). 1990; 15(11):1204–1210.15. Baba I, Murakamu T. Treatment for degenerative spondylolisthesis: the results of semi-circumferential decompression, surgical therapy without fusion. Rinsho Seikei Geka. 1997; 32:1303–1309.16. Okuda T, Baba I, Fujimoto Y, et al. The pathology of ligamentum flavum in degenerative lumbar disease. Spine (Phila Pa 1976). 2004; 29(15):1689–1697.
Article17. Okuda T, Fujimoto Y, Tanaka N, Ishida O, Baba I, Ochi M. Morphological changes of the ligamentum flavum as a cause of nerve root compression. Eur Spine J. 2005; 14(3):277–286.
Article18. Zander T, Rohlmann A, Klockner C, Bergmann G. Influence of graded facetectomy and laminectomy on spinal biomechanics. Eur Spine J. 2003; 12(4):427–434.
Article19. Hamasaki T, Tanaka N, Kim J, Okada M, Ochi M, Hutton WC. Biomechanical assessment of minimally invasive decompression for lumbar spinal canal stenosis: a cadaver study. J Spinal Disord Tech. 2009; 22(7):486–491.
Article20. Abumi K, Panjabi MM, Kramer KM, Duranceau J, Oxland T, Crisco JJ. Biomechanical evaluation of lumbar spinal stability after graded facetectomies. Spine (Phila Pa 1976). 1990; 15(11):1142–1147.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Three types of ligamentum flavum resections for the treatment of lumbar central canal stenosis: BUTTERFLY retrospective study
- Biportal endoscopic en bloc removal of the ligamentum flavum for spinal stenosis: nuances for the “butterfly” technique
- Long Term Clinical and Radiographic Results of Lumbar Spinal Stenosis with Grade I Degenerative Spondylolisthesis after Microsurgical Bilateral Decompression via Unilateral Laminotomy
- Histology of the Ligament Flavumin Degenerative Lumbar Disease
- MR Findings of Spondylolisthesis: Assessment of Associated Spinal and Neural Foraminal Stenosis
