Plunging Ranulas Revisited: A CT Study with Emphasis on a Defect of the Mylohyoid Muscle as the Primary Route of Lesion Propagation
- Affiliations
-
- 1Department of Radiology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul 06351, Korea. hyungkim@skku.edu
- 2Department of Radiology, Hanyang University Hospital, Hanyang University College of Medicine, Seoul 04763, Korea.
- 3Departments of Otorhinolaryngology-Head and Neck Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul 06351, Korea.
- KMID: 2360212
- DOI: http://doi.org/10.3348/kjr.2016.17.2.264
Abstract
OBJECTIVE
The purpose of this study was to clarify the pathogenesis of plunging ranulas in regard of the pathway of lesion propagation using CT scans.
MATERIALS AND METHODS
We retrospectively reviewed CT scans of 41 patients with plunging ranula. We divided plunging ranulas into two types: type 1 was defined as those directly passing through a defect of the mylohyoid muscle with the presence (type 1A) or absence (type 1B) of the tail sign and type 2 as those through the traditional posterior route along the free edge of the mylohyoid muscle. Images were also analyzed for the extent of the lesion in respect to the spaces involved. As for type 1 lesions, we recorded the location of the defect of the mylohyoid muscle and the position of the sublingual gland in relation to the defect.
RESULTS
CT scans demonstrated type 1 lesion in 36 (88%), including type 1A in 14 and type 1B in 22, and type 2 lesion in 5 (12%). Irrespective of the type, the submandibular space was seen to be involved in all cases either alone or in combination with one or more adjacent spaces. Of the 36 patients with type 1 lesions, the anterior one-third was the most common location of the defect of the mylohyoid muscle, seen in 22 patients. The sublingual gland partially herniated in 30 patients.
CONCLUSION
Our results suggest that the majority of plunging ranulas take an anterior shortcut through a defect of the mylohyoid muscle.
Keyword
MeSH Terms
Figure
-
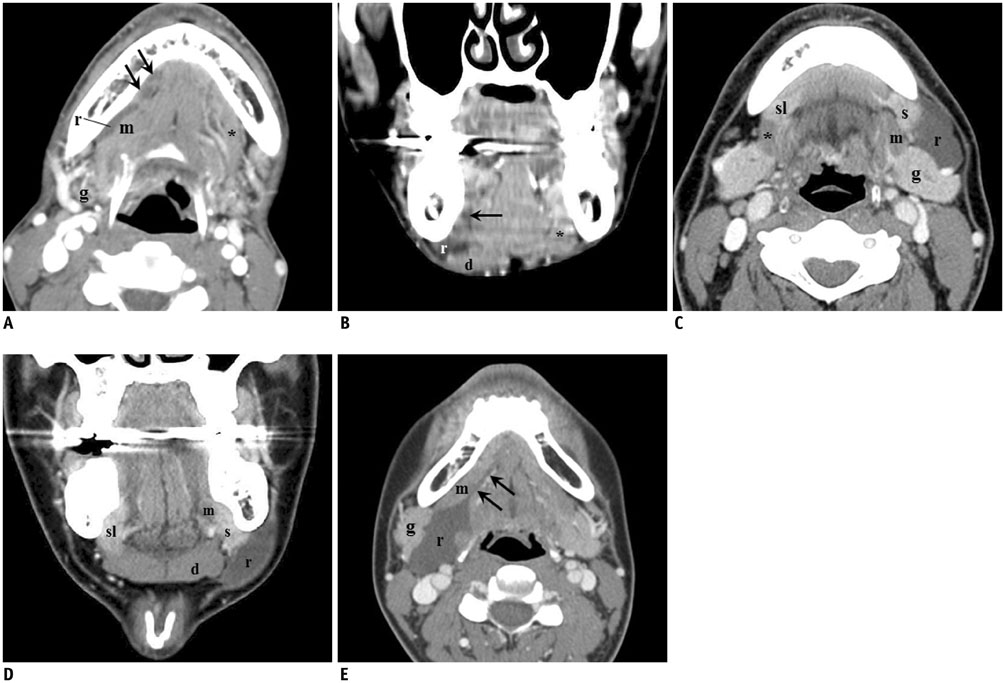
Fig. 1 Classification of plunging ranula. A, B. Type 1A. Contrast-enhanced axial (A) and reformatted coronal (B) CT scans show elongated cystic lesion (r) in right submandibular space (SMS), lateral to mylohyoid muscle (m), which cannot be traced in anterior mouth floor. Instead, small cystic lesions (tail sign, arrows) are seen in ipsilateral sublingual space, contiguous to cystic lesion in SMS. Anterior part of ipsilateral mylohyoid muscle is missing on coronal image, while that on contralateral side (*) is well visualized. C, D. Type 1B. Contrast-enhanced axial (C) and reformatted coronal (D) CT scans show lobulated cystic lesion (r) in left SMS, lateral to mylohyoid muscle (m) and anterior to submandibular gland (g). Cyst abuts sublingual gland (s), which is displaced laterally through anterior defect of mylohyoid muscle, without evidence of tail sign. Also noted is even larger size of anterior defect of contralateral mylohyoid muscle (*), through which sublingual gland (sl) also herniates partially. E. Type 2. Contrast-enhanced axial CT scan shows large lobulated cystic lesion (r) in right SMS, posterior to mylohyoid muscle (m) and medial to submandibular gland (g). Beak with narrow channel directing to sublingual space is noted at anterior portion of cyst (tail sign, arrows). d = digastric muscle
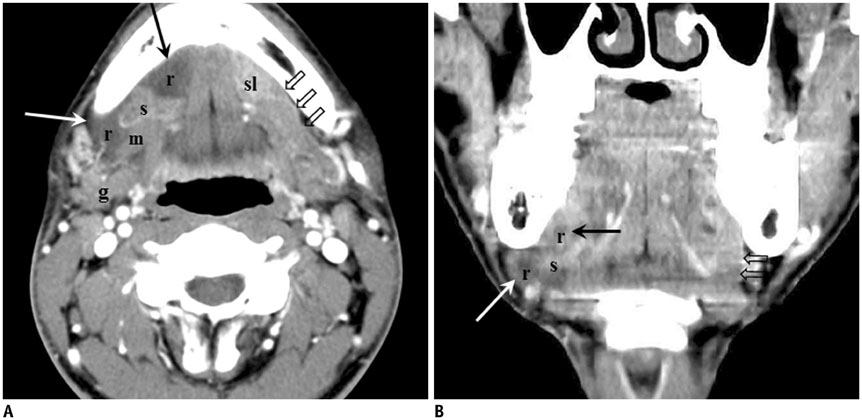
Fig. 2 Type 1A plunging ranula in 23-year-old man. Contrast-enhanced axial (A) and reformatted coronal (B) CT scans show cystic lesion (r) occupying sublingual (black arrows) and submandibular (white arrows) spaces on right through large anterior defect of mylohyoid muscle (m). Sublingual gland (s) also herniates through mylohyoid defect. Within submandibular space, lesion lies anterior to submandibular gland (g). Compare mylohyoid muscle (open arrows) and sublingual gland (sl) in contralateral neck.
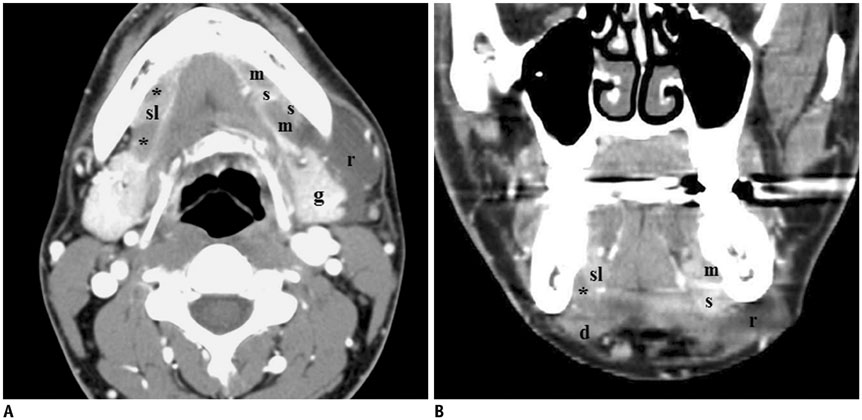
Fig. 3 Type 1B plunging ranula in 26-year-old man. Contrast-enhanced axial (A) and reformatted coronal (B) CT scans show large cystic lesion (r) in left submandibular space (SMS) around angle of mandible. Within SMS, lesion lies anterolateral to submandibular gland (g), contiguous anteromedially to sublingual gland (s) which herniates through defect of mylohyoid muscle (m). Note similar appearance of defect of mylohyoid muscle (*) in contralateral neck. d = digastric muscle, sl = contralateral sublingual gland
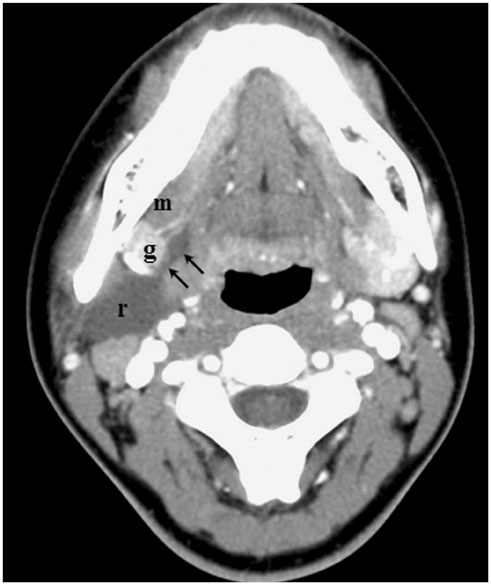
Fig. 4 Type 2 plunging ranula in 17-year-old man. Contrast-enhanced axial CT scan shows cystic lesion (r) in right submandibular space (SMS). Lesion tapers anteromedially toward sublingual space through posterior free edge of mylohyoid muscle (m), creating so-called tail sign (arrows). Within SMS, lesion lies posterior to submandibular gland (g).
Reference
-
1. Macdonald AJ, Salzman KL, Harnsberger HR. Giant ranula of the neck: differentiation from cystic hygroma. AJNR Am J Neuroradiol. 2003; 24:757–761.2. Coit WE, Harnsberger HR, Osborn AG, Smoker WR, Stevens MH, Lufkin RB. Ranulas and their mimics: CT evaluation. Radiology. 1987; 163:211–216.3. Zhao YF, Jia Y, Chen XM, Zhang WF. Clinical review of 580 ranulas. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004; 98:281–287.4. Kurabayashi T, Ida M, Yasumoto M, Ohbayashi N, Yoshino N, Tetsumura A, et al. MRI of ranulas. Neuroradiology. 2000; 42:917–922.5. Charnoff SK, Carter BL. Plunging ranula: CT diagnosis. Radiology. 1986; 158:467–468.6. Hopp E, Mortensen B, Kolbenstvedt A. Mylohyoid herniation of the sublingual gland diagnosed by magnetic resonance imaging. Dentomaxillofac Radiol. 2004; 33:351–353.7. Jain P, Jain R, Morton RP, Ahmad Z. Plunging ranulas: high-resolution ultrasound for diagnosis and surgical management. Eur Radiol. 2010; 20:1442–1449.8. Mair IW, Schewitsch I, Svendsen E, Haugeto OK. Cervical ranula. J Laryngol Otol. 1979; 93:623–628.9. Otonari-Yamamoto M, Nakajima K, Tsuji Y, Otonari T, Curtin HD, Okano T, et al. Imaging of the mylohyoid muscle: separation of submandibular and sublingual spaces. AJR Am J Roentgenol. 2010; 194:W431–W438.10. Davison MJ, Morton RP, McIvor NP. Plunging ranula: clinical observations. Head Neck. 1998; 20:63–68.11. Jain P, Jain R. Types of sublingual gland herniation observed during sonography of plunging ranulas. J Ultrasound Med. 2014; 33:1491–1497.12. White DK, Davidson HC, Harnsberger HR, Haller J, Kamya A. Accessory salivary tissue in the mylohyoid boutonnière: a clinical and radiologic pseudolesion of the oral cavity. AJNR Am J Neuroradiol. 2001; 22:406–412.13. Gaughran GR. Mylohyoid boutonni're and sublingual bouton. J Anat. 1963; 97:565–568.14. Castelli WA, Huelke DF, Celis A. Some basic anatomic features in paralingual space surgery. Oral Surg Oral Med Oral Pathol. 1969; 27:613–621.15. Engel JD, Harn SD, Cohen DM. Mylohyoid herniation: gross and histologic evaluation with clinical correlation. Oral Surg Oral Med Oral Pathol. 1987; 63:55–59.16. Nathan H, Luchansky E. Sublingual gland herniation through the mylohyoid muscle. Oral Surg Oral Med Oral Pathol. 1985; 59:21–23.17. Kiesler K, Gugatschka M, Friedrich G. Incidence and clinical relevance of herniation of the mylohyoid muscle with penetration of the sublingual gland. Eur Arch Otorhinolaryngol. 2007; 264:1071–1074.18. Kim JH. Ultrasound-guided sclerotherapy for benign non-thyroid cystic mass in the neck. Ultrasonography. 2014; 33:83–90.19. Rho MH, Kim DW, Kwon JS, Lee SW, Sung YS, Song YK, et al. OK-432 sclerotherapy of plunging ranula in 21 patients: it can be a substitute for surgery. AJNR Am J Neuroradiol. 2006; 27:1090–1095.
