Ewha Med J.
2016 Oct;39(4):133-136. 10.12771/emj.2016.39.4.133.
Kawasaki Disease with Optic Disc Swelling and Uveitis
- Affiliations
-
- 1Department of Pediatrics, Ewha Womans University School of Medicine, Seoul, Korea. ymhong@ewha.ac.kr
- KMID: 2356387
- DOI: http://doi.org/10.12771/emj.2016.39.4.133
Abstract
- Kawasaki disease (KD) is the self-limited and multisystem vasculitis which accompanies many complications. Ophthalmic findings in KD are bilateral conjunctival injection, iridocyclitis, superficial keratitis, vitreous opacities and subconjunctival hemorrhage. Optic disc swelling is a rare ophthalmic complication in KD. We describe a 3-year-old boy who presented with 7 days of fever, both conjunctival injection without discharge, and right cervical lymph node enlargement of more than 1.5 cm. He was diagnosed as incomplete KD. He had no ocular symptom except bilateral conjunctival injection. On ophthalmic examination, he was diagnosed by anterior uveitis with optic disc swelling. The brain magnetic resonance imaging was performed and revealed no evidence of increased intracranial pressure. Echocardiography revealed the dilated right coronary artery up to 3.4 mm. Fever subsided and optic disc swelling was completely improved after intravenous immunoglobulin (2 g/kg) treatment. Optic disc swelling is a rare ophthalmic complication in KD.
MeSH Terms
Figure
-
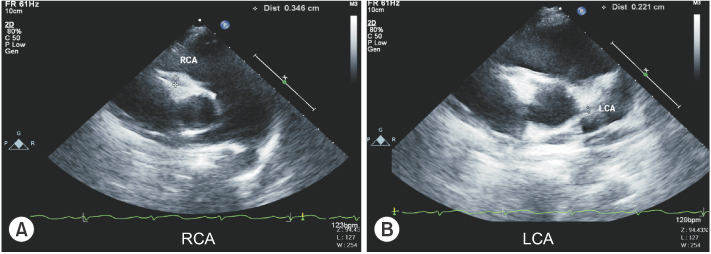
Fig. 1 Two dimensional echocardiographic finding in Kawasaki disease. (A) An echocardiogram reveals dilatation of right coronary artery. (B) Left coronary artery is normal. RCA, right coronary artery; LCA, left coronary artery.
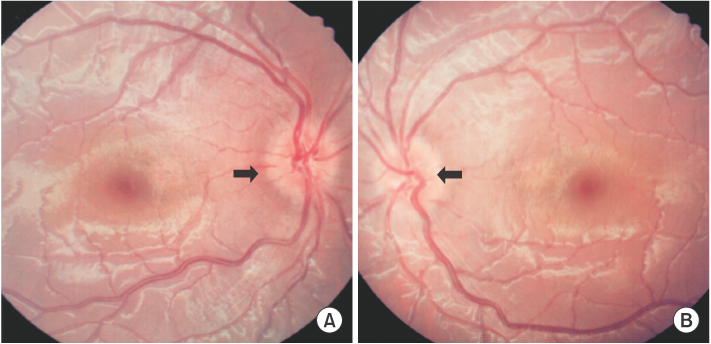
Fig. 2 Ophthalmoscopic examination in Kawasaki disease patient. This figure shows optic disc margin blunting of 360-degree in both eyes (A, B). The arrows indicate the optic disc margin blunting. A, right eye; B, left eye.
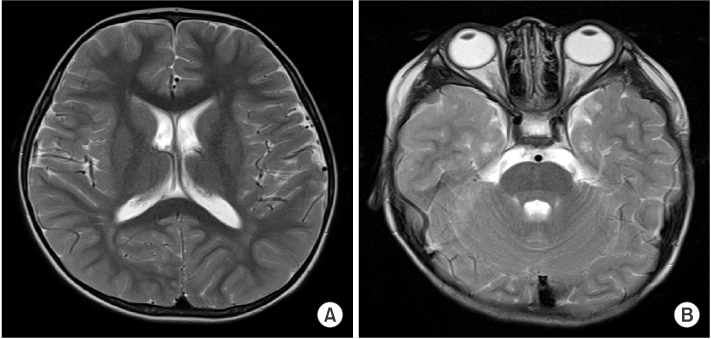
Fig. 3 Brain magnetic resonance imaging (T2-weighted axial scan). There is no evidence of abnormal signal lesion in the brain. No abnormal enhancing lesion is seen (A, B). A, Thalamus-basal ganglia level; B, Pons level.
Reference
-
1. Newburger JW, Takahashi M, Gerber MA, Gewitz MH, Tani LY, Burns JC, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a statement for health professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Pediatrics. 2004; 114:1708–1733.2. Bae HK, Lee DK, Kwon JH, Kim HS, Sohn S, Hong YM. Clinical characteristics and serum N-terminal pro-brain natriuretic peptide as a diagnostic marker of Kawasaki disease in infants younger than 3 months of age. Korean J Pediatr. 2014; 57:357–362.3. Freeman AF, Shulman ST. Kawasaki disease: summary of the American Heart Association guidelines. Am Fam Physician. 2006; 74:1141–1148.4. Grouteau E, Debuisson C, Brochard K, Paranon S, Lesage Beaudon C, Pajot C, et al. Severe global inflammatory involvement of ocular segments and optic disc swelling in a 12-year-old girl with Kawasaki disease. Eur J Ophthalmol. 2011; 21:112–114.5. Choi HS, Lee SB, Kwon JH, Kim HS, Sohn S, Hong YM. Uveitis as an important ocular sign to help early diagnosis in Kawasaki disease. Korean J Pediatr. 2015; 58:374–379.6. Alves NR, Magalhaes CM, Almeida Rde F, Santos RC, Gandolfi L, Pratesi R. Prospective study of Kawasaki disease complications: review of 115 cases. Rev Assoc Med Bras. 2011; 57:295–300.7. Guney E, Tugal-Tutkun I. Symptoms and signs of anterior uveitis. US Ophthalmic Rev. 2013; 6:33–37.8. Anand S, Yang YC. Optic disc changes in Kawasaki disease. J Pediatr Ophthalmol Strabismus. 2004; 41:177–179.9. Kovarik JJ, Doshi PN, Collinge JE, Plager DA. Outcome of pediatric patients referred for papilledema. J AAPOS. 2015; 19:344–348.10. Kadyan A, Choi J, Headon MP. Disciform keratitis and optic disc swelling in Kawasaki disease: an unusual presentation. Eye (Lond). 2006; 20:976–977.11. Ohno S, Miyajima T, Higuchi M, Yoshida A, Matsuda H, Saheki Y, et al. Ocular manifestations of Kawasaki’s disease (mucocutaneous lymph node syndrome). Am J Ophthalmol. 1982; 93:713–717.12. Foster CS, Kothari S, Anesi SD, Vitale AT, Chu D, Metzinger JL, et al. The Ocular Immunology and Uveitis Foundation preferred practice patterns of uveitis management. Surv Ophthalmol. 2016; 61:1–17.13. Burns JC, Joffe L, Sargent RA, Glode MP. Anterior uveitis associated with Kawasaki syndrome. Pediatr Infect Dis. 1985; 4:258–261.14. Rogers DL. A review of pediatric idiopathic intracranial hypertension. Pediatr Clin North Am. 2014; 61:579–590.15. Patel RM, Shulman ST. Kawasaki disease: a comprehensive review of treatment options. J Clin Pharm Ther. 2015; 40:620–625.
