Clinical importance of congenital anomalies of the inferior vena cava in organ procurement surgery from a deceased donor: two case reports
- Affiliations
-
- 1Division of Vascular and Transplantation Surgery, Department of Surgery, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea. cmckji@catholic.ac.kr
- KMID: 2356377
- DOI: http://doi.org/10.4174/astr.2016.91.5.260
Abstract
- Congenital anomalies of the inferior vena cava (IVC) are rare but important problems in living donors for kidney transplantation, especially in cases of a short left renal vein and accompanying vascular and urological anatomic variations. However, the clinical impacts of IVC anomalies in deceased donors have yet to be reported. The unexpected presence of an IVC in an unusual position poses challenges to surgeons and increases the risk of bleeding during organ removal. Accompanying vascular variations can cause unexpected bleeding and injury and therefore technical complications in procurement and subsequent implantation. During cold perfusion, inadequate venous drainage or insufficient cooling can induce graft damage. Our cases highlight the need for all transplant surgeons to confirm the anatomy of the aorta, IVC, and major vessels early in the surgical procedure and, should an anomaly be detected, know how to manage the problem.
Keyword
MeSH Terms
Figure
-
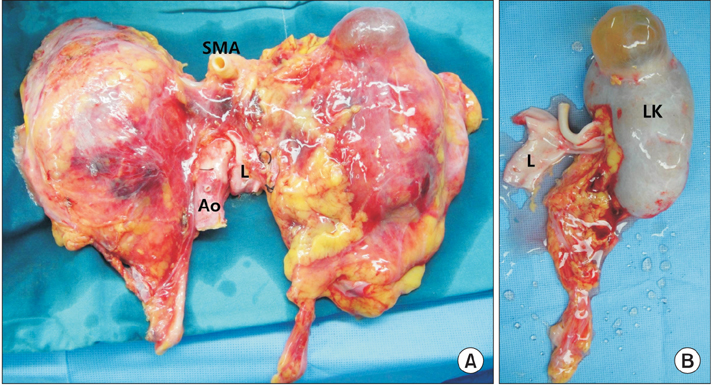
Fig. 1 Kidneys from deceased donor with left-sided inferior vena cava (IVC). (A) Renal grafts after en bloc procurement. Left-sided IVC joined the left renal vein and crossed the aorta anteriorly and then joined the right renal vein. Left renal vein was shorter than the right one. Both kidneys had a single artery. (B) The left kidney was procured together with the IVC. The left renal vein is extended during a back-table procedure using the IVC. L, left-sided IVC; Ao, aorta; SMA, superior mesenteric artery; LK, left kidney.
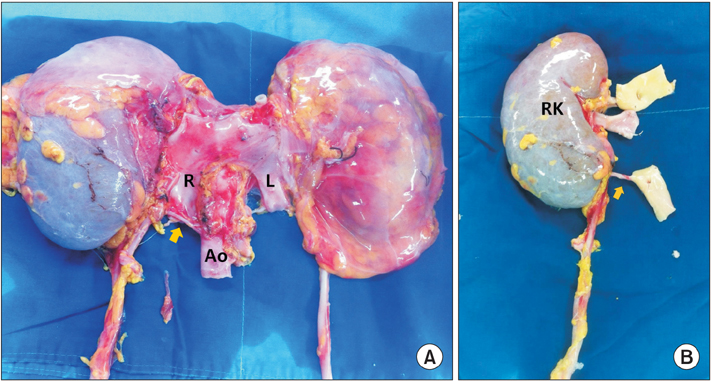
Fig. 2 Kidneys from deceased donor with double inferior vena cava (IVC). (A) Right IVC and second left IVC were identified. Left IVC crossed the aorta just after its union with the left renal vein and then joined the right IVC to form a single, right-sided IVC. The right kidney had double renal arteries (arrow, inferior polar artery arising from aorta) but there were no other anatomic variations. (B) Right kidney after back-table procedure. Right renal vein is extended with IVC. R, right-sided IVC; L, left-sided IVC; Ao, aorta; RK, right kidney.
Reference
-
1. Reis RH, Esenther G. Variations in the pattern of renal vessels and their relation to the type of posterior vena cava in man. Am J Anat. 1959; 104:295–318.2. Aljabri B, MacDonald PS, Satin R, Stein LS, Obrand DI, Steinmetz OK. Incidence of major venous and renal anomalies relevant to aortoiliac surgery as demonstrated by computed tomography. Ann Vasc Surg. 2001; 15:615–618.3. Morita S, Higuchi M, Saito N, Mitsuhashi N. Pelvic venous variations in patients with congenital inferior vena cava anomalies: classification with computed tomography. Acta Radiol. 2007; 48:974–979.4. Sakai H, Ide K, Ishiyama K, Onoe T, Tazawa H, Hotta R, et al. Renal vein extension using an autologous renal vein in a living donor with double inferior vena cava: a case report. Transplant Proc. 2012; 44:1446–1449.5. Ang WC, Doyle T, Stringer MD. Left-sided and duplicate inferior vena cava: a case series and review. Clin Anat. 2013; 26:990–1001.6. Bass JE, Redwine MD, Kramer LA, Huynh PT, Harris JH Jr. Spectrum of congenital anomalies of the inferior vena cava: cross-sectional imaging findings. Radiographics. 2000; 20:639–652.7. Davari HR, Malek-Hosseini SA, Salahi H, Bahador A, Nikeghbalian S, Jalaeian H, et al. Management of infrarenal duplicated inferior vena cava during living related kidney transplantation. Transpl Int. 2007; 20:478–479.8. Ichikawa T, Kawada S, Koizumi J, Endo J, Iino M, Terachi T, et al. Major venous anomalies are frequently associated with horseshoe kidneys. Circ J. 2011; 75:2872–2877.9. Gayer G, Luboshitz J, Hertz M, Zissin R, Thaler M, Lubetsky A, et al. Congenital anomalies of the inferior vena cava revealed on CT in patients with deep vein thrombosis. AJR Am J Roentgenol. 2003; 180:729–732.10. Yang BZ, Li Z, Wang ZG. Nutcracker syndrome due to left-sided inferior vena cava compression and treated with superior mesenteric artery transposition. J Vasc Surg. 2012; 56:816–818.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Kidney transplant in a pediatric patient with double inferior vena cava: a case report
- Transposition of inferior vena cava
- A Case of Congenital Absence of the Inferior Vena Cava
- Venous Stasis and Ulceration Due to Congenital Absence of Inferior Vena Cava
- A case of hemiazygos continuation of a left inferior vena cava
