Endovascular Treatment of Symptomatic Vertebral Artery Dissecting Aneurysms
- Affiliations
-
- 1Department of Neurosurgery, Korea University Ansan Hospital, Ansan, Korea. djlim@korea.ac.kr
- 2Department of Neurosurgery, Hallym University Kangnam Sacred Heart Hospital, Seoul, Korea.
- KMID: 2355642
- DOI: http://doi.org/10.7461/jcen.2016.18.3.201
Abstract
OBJECTIVE
Vertebral artery dissecting aneurysms (VADAs) are rare and many debates are present about treatment options. We review types and efficacy of our endovascular treatments and establish a safe endovascular therapeutic strategy regard to the angio-architecture of VADAs.
MATERIALS AND METHODS
Between July 2008 and October 2015, we treated 22 patients with symptomatic VADAs. Fifteen patients presented with subarachnoid hemorrhage from the ruptured VADAs, digital subtraction angiography and magnetic resonance image confirmed the diagnosis and endovascular treatments were followed as their angio-architecture.
RESULTS
Clinical results were good in 13 patients (86.7%), and there were no technical problems during endovascular procedures. The other 2 patients with poor prognosis showed severe neurological deficits at the initial evaluation. Among the three different endovascular treatments, there were no radiologic cure in one patient with stent insertion alone, but the patient had no significant clinical symptoms either.
CONCLUSION
Endovascular treatments are safe and effective treatment option for managing VADAs and can be the first treatment of choice for most patients. To select proper endovascular treatment according to the angio-architecture of VADAs can reduce the risk of the treatment.
Keyword
MeSH Terms
Figure
-
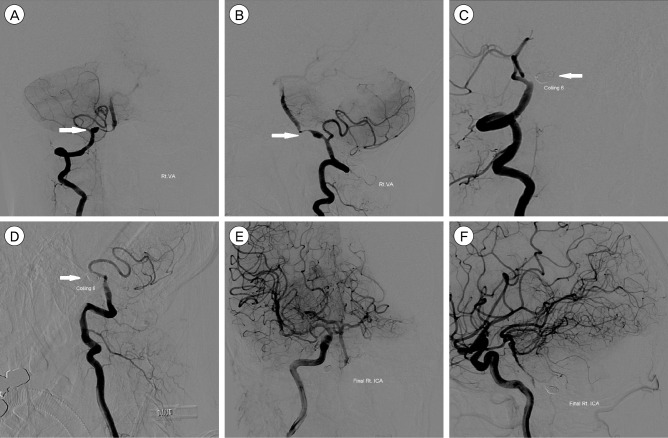
Fig. 1 Digital subtraction angiography (DSA) images of a 39-year-old woman presented with subarachnoid hemorrhage (SAH). The anterior-posterior (AP) and lateral view of the right vertebral angiogram shows a vertebral artery dissecting aneurysm (VADA) presented with "pearl and string sign", which is located at the distal to the origin of the posterior inferior cerebellar artery (PICA) (A, B; white arrow). Vertebral artery coil trapping technic was performed, and a total of 6 detachable coils, 37 cm in length, were placed into the dissecting segment and proximal parent artery, resulting in complete occlusion of the dissecting aneurysm with preservation of PICA flow (C, D; white arrow shows complete embolization of the VADA). The AP and lateral view of the right internal carotid angiogram shows sufficient collateral flow via right posterior communicating artery to the vertebrobasilar system without retrograde filling of the VADA (E, F).
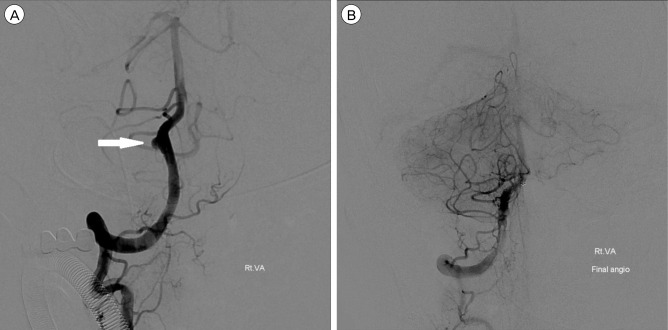
Fig. 2 DSA images of a 51-year-old man presented with SAH and IVH. The lateral view of the right vertebral angiogram shows a VADA presented with "saccular aneurysm with wide neck" (A; white arrow). Double stent assisted coil embolization technic was performed, and a total of 4 detachable coils, 12 cm in length, were placed into the aneurysmal sac, resulting in near complete occlusion of the dissecting aneurysm with preservation of PICA and distal flow (B). DSA = Digital Subtraction Angiography; SAH = subarachnoid hemorrhage; IVH = intraventricular hemorrhage; VADA = vertebral artery dissecting aneurysm; PICA = posterior inferior cerebellar artery.
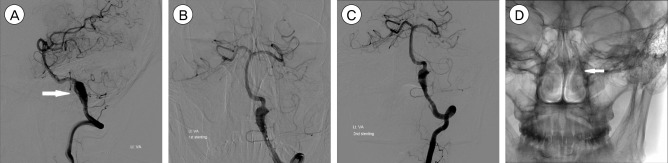
Fig. 3 DSA images of a 45-year-old man presented with SAH. The lateral view of the left vertebral angiogram shows a VADA presented with "fusiform dilation" (A; white arrow). Stent insertion alone technic was performed due to the balloon occlusion test was positive, and 2 stents were placed into the dissecting segment, resulting in incomplete occlusion of the dissecting aneurysm (B, C). The AP view of skull x-ray after stent insertion shows 2 stents are overlapped and well placed (D; white arrow). DSA = Digital Subtraction Angiography; SAH = subarachnoid hemorrhage; VADA = vertebral artery dissecting aneurysm.
Cited by 1 articles
-
A Ruptured Vertebral Artery Dissecting Aneurysm that Grew Immediately: Case Report
Jung Hyun Park
Kosin Med J. 2021;36(2):211-216. doi: 10.7180/kmj.2021.36.2.211.
Reference
-
1. Andoh T, Shirakami S, Nakashima T, Nishimura Y, Sakai N, Yamada H, et al. Clinical analysis of a series of vertebral aneurysm cases. Neurosurgery. 1992; 12. 31(6):987–993. PMID: 1470333.
Article2. Aoki N, Sakai T. Rebleeding from intracranial dissecting aneurysm in the vertebral artery. Stroke. 1990; 11. 21(11):1628–1631. PMID: 2237959.
Article3. Arnold M, Bousser MG, Fahrni G, Fischer U, Georgiadis D, Gandjour J, et al. Vertebral artery dissection: presenting findings and predictors of outcome. Stroke. 2006; 10. 37(10):2499–2503. PMID: 16960096.4. Kim MS. Endovascular coil trapping of a ruptured dissecting aneurysm of the vertebral artery using detachable coils and micro tornado® coils. J Cerebrovasc Endovasc Neurosurg. 2013; 6. 15(2):96–101. PMID: 23844353.5. Luo C-B, Chang CY, Teng MM, Chang FC. Endovascular treatment of ruptured vertebral dissecting aneurysms with electrodetachable coils. J Chin Med Assoc. 2005; 12. 68(12):578–584. PMID: 16379342.
Article6. Lylyk P, Ceratto R, Hurvitz D, Basso A. Treatment of a vertebral dissecting aneurysm with stents and coils: technique and case report. Neurosurgery. 1998; 8. 43(2):385–388. PMID: 9696097.7. Mizutani T, Aruga T, Kirino T, Miki Y, Saito I, Tsuchida T. Recurrent subarachnoid hemorrhage from untreated ruptured vertebrobasilar dissecting aneurysms. Neurosurgery. 1995; 5. 36(5):905–911. discussion 912-3. PMID: 7791980.
Article8. Nashimoto T, Komata T, Honma J, Yamashita S, Seki Y, Kurashima A, et al. Successful treatment of bilateral vertebral artery dissecting aneurysms with subarachnoid hemorrhage: report of three cases. J Stroke Cerebrovasc Dis. 2012; 7. 21(5):422–427. PMID: 21111633.
Article9. Peluso JP, van Rooij WJ, Sluzewski M, Beute GN, Majoie CB. Endovascular treatment of symptomatic intradural vertebral dissecting aneurysms. AJNR Am J Neuroradiol. 2008; 1. 29(1):102–106. PMID: 17928377.
Article10. Taha MM, Sakaida H, Asakura F, Maeda M, Toma N, Yamamoto A, et al. Endovascular management of vertebral artery dissecting aneurysms: review of 25 patients. Turk Neurosurg. 2010; 4. 20(2):126–135. PMID: 20401839.
Article11. Wang Y, Zhao C, Hao X, Wang C, Wang Z. Endovascular interventional therapy and classification of vertebral artery dissecting aneurysms. Exp Ther Med. 2014; 11. 8(5):1409–1415. PMID: 25289031.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endovascular Surgery of Vertebral Artery Dissecting Aneurysm
- A Case of Endovascular Treatment for Followed by Side to Side Bypass for Vertebral Artery Dissecting Aneurysms Involved Posterior Inferior Cerebellar Artery
- Growing Thrombosed Dissecting Aneurysm of the Vertebral Artery after Endovascular Proximal Artery Occlusion: the Role of the Vasa Vasorum
- Endovascular Coil Trapping of a Ruptured Dissecting Aneurysm of the Vertebral Artery Using Detachable Coils and Micro-Tornado(R) Coils
- Bilateral Vertebral Artery Dissecting Aneurysms: A Long Term Follow-up Results of Microsurgical Trapping and Proximal Occlusion
