J Korean Med Sci.
2016 Dec;31(12):1929-1936. 10.3346/jkms.2016.31.12.1929.
Clinical Outcomes in Patients with Deferred Coronary Lesions according to Disease Severity Assessed by Fractional Flow Reserve
- Won KB

- Nam CW
- Cho YK
- Yoon HJ
- Park HS
- Kim H
- Han S
- Hur SH
- Kim YN
- Park SH
- Han JK
- Koo BK
- Kim HS
- Doh JH
- Lee SY
- Yang HM
- Lim HS
- Yoon MH
- Tahk SJ
- Kim KB
- Affiliations
-
- 1Division of Cardiology, Keimyung University Dongsan Medical Center, Daegu, Korea. ncwcv@dsmc.or.kr
- 2Division of Cardiology, Ulsan University Hospital, Ulsan, Korea.
- 3Division of Cardiology, Eulji University Hospital, Daejeon, Korea.
- 4Division of Cardiology, Seoul National University Hospital, Seoul, Korea.
- 5Division of Cardiology, Inje University Ilsan Paik Hospital, Goyang, Korea.
- 6Division of Cardiology, Ajou University Medical Center, Suwon, Korea.
- KMID: 2355621
- DOI: http://doi.org/10.3346/jkms.2016.31.12.1929
Abstract
- Data on the clinical outcomes in deferred coronary lesions according to functional severity have been limited. This study evaluated the clinical outcomes of deferred lesions according to fractional flow reserve (FFR) grade using Korean FFR registry data. Among 1,294 patients and 1,628 lesions in Korean FFR registry, 665 patients with 781 deferred lesions were included in this study. All participants were consecutively categorized into 4 groups according to FFR; group 1: ≥ 0.96 (n = 56), group 2: 0.86-0.95 (n = 330), group 3: 0.81-0.85 (n = 170), and group 4: ≤ 0.80 (n = 99). Primary endpoint was major adverse cardiac events (MACE), a composite of all-cause death, myocardial infarction, and target vessel revascularization. The median follow-up period was 2.1 years. During follow-up, the incidence of MACE in groups 1-4 was 1.8%, 7.6%, 8.8%, and 13.1%, respectively. Compared to group 1, the cumulative rate by Kaplan-Meier analysis of MACE was not different for groups 2 and 3. However, group 4 had higher cumulative rate of MACE compared to group 1 (log-rank P = 0.013). In the multivariate Cox hazard models, only FFR (hazard ratio [HR], 0.95; P = 0.005) was independently associated with MACE among all participants. In contrast, previous history of percutaneous coronary intervention (HR, 2.37; P = 0.023) and diagnosis of acute coronary syndrome (ACS) (HR, 2.35; P = 0.015), but not FFR, were independent predictors for MACE in subjects with non-ischemic (FFR ≥ 0.81) deferred coronary lesions. Compared to subjects with ischemic deferred lesions, clinical outcomes in subjects with non-ischemic deferred lesions according to functional severity are favorable. However, longer-term follow-up may be necessary.
MeSH Terms
Figure
-
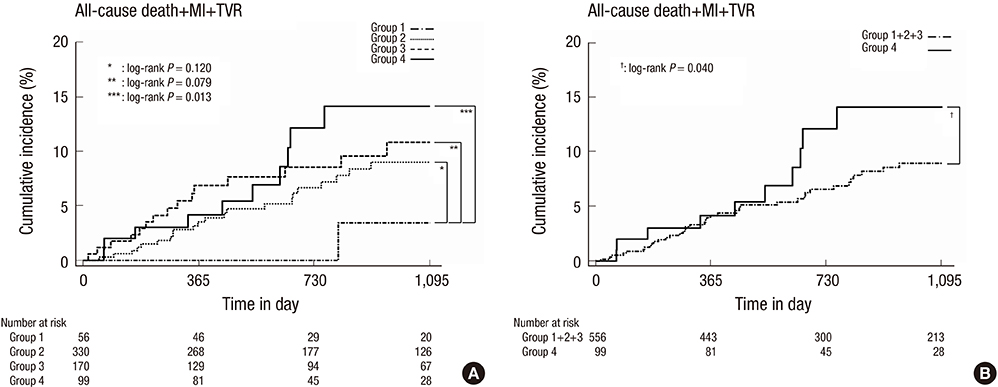
Fig. 1 Time-to-event curve for 3-year MACE. Comparison of the event of MACE based on (A) normal FFR and (B) FFR < 0.80. MACE = major adverse cardiac events, FFR = fractional flow reserve, MI = myocardial infarction, TVR = target vessel revascularization. *log-rank P = 0.120; †log-rank P = 0.079; ‡log-rank P = 0.013; §log-rank P = 0.040.
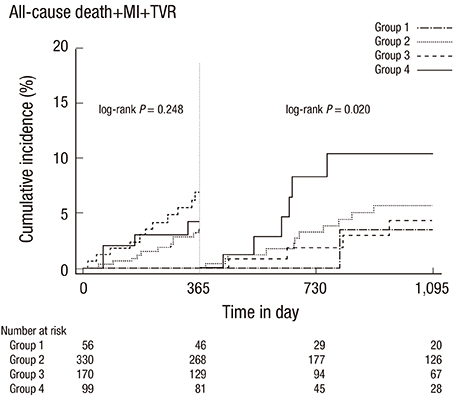
Fig. 2 One-year landmark analysis for MACE. MACE = major adverse cardiac events, MI = myocardial infarction, TVR = target vessel revascularization.
Reference
-
1. Burggraf GW, Parker JO. Prognosis in coronary artery disease. Angiographic, hemodynamic, and clinical factors. Circulation. 1975; 51:146–156.2. Stone GW, Maehara A, Lansky AJ, de Bruyne B, Cristea E, Mintz GS, Mehran R, McPherson J, Farhat N, Marso SP, et al. A prospective natural-history study of coronary atherosclerosis. N Engl J Med. 2011; 364:226–235.3. Yun KH, Mintz GS, Farhat N, Marso SP, Taglieri N, Verheye S, Foster MC, Margolis MP, Templin B, Xu K, et al. Relation between angiographic lesion severity, vulnerable plaque morphology and future adverse cardiac events (from the providing regional observations to study predictors of events in the coronary tree study). Am J Cardiol. 2012; 110:471–477.4. Pijls NH, van Schaardenburgh P, Manoharan G, Boersma E, Bech JW, van’t Veer M, Bär F, Hoorntje J, Koolen J, Wijns W, et al. Percutaneous coronary intervention of functionally nonsignificant stenosis: 5-year follow-up of the DEFER study. J Am Coll Cardiol. 2007; 49:2105–2111.5. Tonino PA, De Bruyne B, Pijls NH, Siebert U, Ikeno F. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N Engl J Med. 2009; 360:213–224.6. Nam CW, Yoon HJ, Cho YK, Park HS, Kim H, Hur SH, Kim YN, Chung IS, Koo BK, Tahk SJ, et al. Outcomes of percutaneous coronary intervention in intermediate coronary artery disease: fractional flow reserve-guided versus intravascular ultrasound-guided. JACC Cardiovasc Interv. 2010; 3:812–817.7. De Bruyne B, Pijls NH, Kalesan B, Barbato E, Tonino PA, Piroth Z, Jagic N, Möbius-Winkler S, Rioufol G, Witt N, et al. Fractional flow reserve-guided PCI versus medical therapy in stable coronary disease. N Engl J Med. 2012; 367:991–1001.8. Doh JH, Nam CW, Koo BK, Park SH, Lee JH, Han JK, Yang HM, Lim HS, Yoon MH, Cho YK, et al. Long-term patient-related and lesion-related outcomes after real-world fractional flow reserve use. J Invasive Cardiol. 2015; 27:410–415.9. Kushner FG, Hand M, Smith SC Jr, King SB 3rd, Anderson JL, Antman EM, Bailey SR, Bates ER, Blankenship JC, Casey DE Jr, et al. 2009 focused updates: ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction (updating the 2004 guideline and 2007 focused update) and ACC/AHA/SCAI guidelines on percutaneous coronary intervention (updating the 2005 guideline and 2007 focused update): a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation. 2009; 120:2271–2306.10. Pijls NH, De Bruyne B, Peels K, Van Der Voort PH, Bonnier HJ, Bartunek J, Koolen JJ. Measurement of fractional flow reserve to assess the functional severity of coronary-artery stenoses. N Engl J Med. 1996; 334:1703–1708.11. De Bruyne B, Pijls NH, Barbato E, Bartunek J, Bech JW, Wijns W, Heyndrickx GR. Intracoronary and intravenous adenosine 5′-triphosphate, adenosine, papaverine, and contrast medium to assess fractional flow reserve in humans. Circulation. 2003; 107:1877–1883.12. Yoon MH, Tahk SJ, Yang HM, Park JS, Zheng M, Lim HS, Choi BJ, Choi SY, Choi UJ, Hwang JW, et al. Comparison of the intracoronary continuous infusion method using a microcatheter and the intravenous continuous adenosine infusion method for inducing maximal hyperemia for fractional flow reserve measurement. Am Heart J. 2009; 157:1050–1056.13. Seo MK, Koo BK, Kim JH, Shin DH, Yang HM, Park KW, Lee HY, Kang HJ, Kim HS, Oh BH, et al. Comparison of hyperemic efficacy between central and peripheral venous adenosine infusion for fractional flow reserve measurement. Circ Cardiovasc Interv. 2012; 5:401–405.14. Austen WG, Edwards JE, Frye RL, Gensini GG, Gott VL, Griffith LS, McGoon DC, Murphy ML, Roe BB. A reporting system on patients evaluated for coronary artery disease. Report of the Ad Hoc Committee for grading of coronary artery disease, Council on Cardiovascular Surgery, American Heart Association. Circulation. 1975; 51:5–40.15. Thygesen K, Alpert JS, White HD. Universal definition of myocardial infarction. Circulation. 2007; 116:2634–2653.16. Hachamovitch R, Hayes SW, Friedman JD, Cohen I, Berman DS. Comparison of the short-term survival benefit associated with revascularization compared with medical therapy in patients with no prior coronary artery disease undergoing stress myocardial perfusion single photon emission computed tomography. Circulation. 2003; 107:2900–2907.17. Boden WE, O’Rourke RA, Teo KK, Hartigan PM, Maron DJ, Kostuk WJ, Knudtson M, Dada M, Casperson P, Harris CL, et al. Optimal medical therapy with or without PCI for stable coronary disease. N Engl J Med. 2007; 356:1503–1516.18. Johnson NP, Tóth GG, Lai D, Zhu H, Açar G, Agostoni P, Appelman Y, Arslan F, Barbato E, Chen SL, et al. Prognostic value of fractional flow reserve: linking physiologic severity to clinical outcomes. J Am Coll Cardiol. 2014; 64:1641–1654.19. Shiono Y, Kubo T, Tanaka A, Ino Y, Yamaguchi T, Tanimoto T, Yamano T, Matsuo Y, Nishiguchi T, Teraguchi I, et al. Long-term outcome after deferral of revascularization in patients with intermediate coronary stenosis and gray-zone fractional flow reserve. Circ J. 2015; 79:91–95.20. Yamashita J, Tanaka N, Shindo N, Ogawa M, Kimura Y, Sakoda K, Murata N, Hokama Y, Hoshino K, Ikeda S, et al. Seven-year clinical outcomes of patients with moderate coronary artery stenosis after deferral of revascularization based on gray-zone fractional flow reserve. Cardiovasc Interv Ther. 2015; 30:209–215.21. Depta JP, Patel JS, Novak E, Masrani SK, Raymer D, Facey G, Patel Y, Zajarias A, Lasala JM, Singh J, et al. Outcomes of coronary stenoses deferred revascularization for borderline versus nonborderline fractional flow reserve values. Am J Cardiol. 2014; 113:1788–1793.22. Depta JP, Patel JS, Novak E, Gage BF, Masrani SK, Raymer D, Facey G, Patel Y, Zajarias A, Lasala JM, et al. Risk model for estimating the 1-year risk of deferred lesion intervention following deferred revascularization after fractional flow reserve assessment. Eur Heart J. 2015; 36:509–515.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Funtional significance of the intermediate lesion in a single coronary artery assessed by fractional flow reserve
- Percutaneous coronary intervention in patients with multi-vessel coronary artery disease: a focus on physiology
- Fractional Flow Reserve: The Past, Present and Future
- Physiologic approach for coronary intervention
- Fractional Flow Reserve in Coronary Artery Disease: Comparison with Intravascular Ultrasound
