Korean Circ J.
2016 Nov;46(6):866-869. 10.4070/kcj.2016.46.6.866.
Complete Heart Block in Association with Dengue Hemorrhagic Fever
- Affiliations
-
- 1Department of Medicine, Mount Sinai St. Luke's and Mount Sinai Roosevelt Hospitals, Icahn School of Medicine, New York, NY, USA.
- 2Department of Medicine, New York-Presbyterian Hospital, Weill Cornell Medical College, New York, NY, USA. faisalinayat@hotmail.com
- 3Department of Medicine, Johnson City Medical Center, Quillen College of Medicine, Johnson City, TN, USA.
- KMID: 2355465
- DOI: http://doi.org/10.4070/kcj.2016.46.6.866
Abstract
- Dengue virus infection affects the heart structurally and functionally. Clinical manifestations of cardiac complications secondary to dengue virus infection vary from self-limiting arrhythmias to severe myocardial infarction, leading to hypotension, pulmonary edema, and cardiogenic shock. However, we report a case of dengue hemorrhagic fever (DHF) complicated by a complete heart block. A female with DHF due to dengue virus serotype 2, presented to the emergency department with fever, headache, rash, and fatigue followed by an episode of syncope. She was found to have a third-degree atrioventricular block, with pulseless polymorphic ventricular tachycardia. Patient was resuscitated and a temporary trans-venous pacemaker was placed. She reverted back to normal sinus rhythm after 4 days of syncope and was subsequently discharged from the hospital after complete resolution of symptoms, without the need for a permanent pacemaker. Physicians are warranted to have high index of suspicion for dengue virus infection as an etiology in patients with acute cardiovascular compromise, especially in tropical areas.
Keyword
MeSH Terms
Figure
-
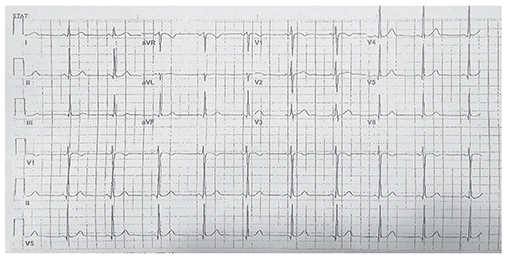
Fig. 1 Baseline normal sinus rhythm.
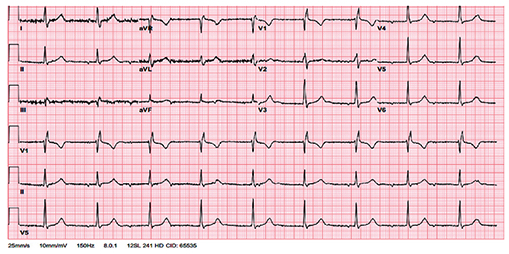
Fig. 2 Complete/third-degree heart block following syncopal attack.
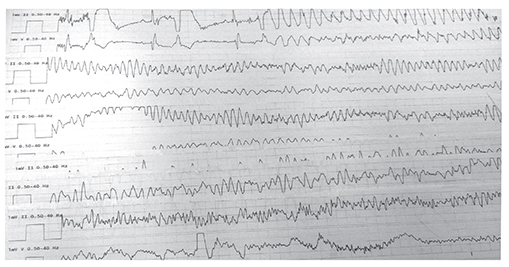
Fig. 3 Polymorphic ventricular tachycardia (V-tach) without pulse.
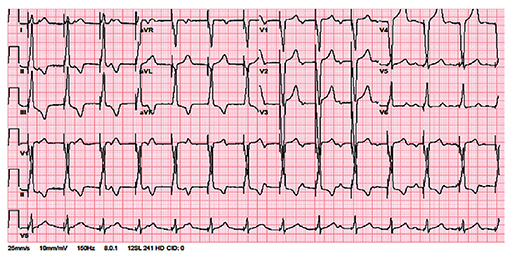
Fig. 4 After achieving return of spontaneous circulation and placing temporary trans-venous pacemaker.
Reference
-
1. Bhatt S, Gething PW, Brady OJ, et al. The global distribution and burden of dengue. Nature. 2013; 496:504–507.2. Teixeira MG, Barreto ML. Diagnosis and management of dengue. BMJ. 2009; 339:b4338.3. Satarasinghe RL, Arultnithy K, Amerasena NL, Bulugahapitiya U, Sahayam DV. Asymptomatic myocardial involvement in acute dengue virus infection in a cohort of adult Sri Lankans admitted to a tertiary referral centre. Br J Cardiol. 2007; 14:171–173.4. Lateef A, Fisher DA, Tambyah PA. Dengue and relative bradycardia. Emerg Infect Dis. 2007; 13:650–651.5. Horta Veloso H, Ferreira Júnior JA, Braga de Paiva JM, et al. Acute atrial fibrillation during dengue hemorrhagic fever. Braz J Infect Dis. 2003; 7:418–422.6. Khongphatthallayothin A, Chotivitayatarakorn P, Somchit S, Mitprasart A, Sakolsattayadorn S, Thisyakorn C. Morbitz type I second degree AV block during recovery from dengue hemorrhagic fever. Southeast Asian J Trop Med Public Health. 2000; 31:642–645.7. Chuah SK. Transient ventricular arrhythmia as a cardiac manifestation in dengue haemorrhagic fever--a case report. Singapore Med J. 1987; 28:569–572.8. Kularatne SA, Pathirage MM, Kumarasiri PV, Gunasena S, Mahindawanse SI. Cardiac complications of a dengue fever outbreak in Sri Lanka, 2005. Trans R Soc Trop Med Hyg. 2007; 101:804–808.9. Lee CH, Teo C, Low AF. Fulminant dengue myocarditis masquerading as acute myocardial infarction. Int J Cardiol. 2009; 136:e69–e71.10. Khongphatthanayothin A, Lertsapcharoen P, Supachokchaiwattana P, et al. Myocardial depression in dengue hemorrhagic fever: prevalence and clinical description. Pediatr Crit Care Med. 2007; 8:524–529.11. Agarwal R, Kapoor S, Nagar R, et al. A clinical study of the patients with dengue hemorrhagic fever during the epidemic of 1996 at Lucknow, India. Southeast Asian J Trop Med Public Health. 1999; 30:735–740.12. Wali JP, Biswas A, Chandra S, et al. Cardiac involvement in dengue haemorrhagic fever. Int J Cardiol. 1998; 64:31–36.13. Lim SMS, Hoo FK, Sulaiman WAW. A case of dengue hemorrhagic fever with myocarditis and complete heart block. RMJ. 2014; 39:104–106.14. Martha JW. Total atrioventricular block due to Dengue myocarditis. J Cardiovasc Electrophysiol. 2009; 20(S59):1045–3873.15. La-Orkhun V, Supachokchaiwattana P, Lertsapcharoen P, Khongphatthanayothin A. Spectrum of cardiac rhythm abnormalities and heart rate variability during the convalescent stage of dengue virus infection: a Holter study. Ann Trop Paediatr. 2011; 31:123–128.16. Tisoncik JR, Korth MJ, Simmons CP, Farrar J, Martin TR, Katze MG. Into the eye of the cytokine storm. Microbiol Mol Biol Rev. 2012; 76:16–32.17. Nijjer S, Ghosh AK, Dubrey SW. Hypocalcaemia, long QT interval and atrial arrhythmias. BMJ Case Rep. 2010; 2010:bcr0820092216.18. Mekmullica J, Suwanphatra A, Thienpaitoon H, et al. Serum and urine sodium levels in dengue patients. Southeast Asian J Trop Med Public Health. 2005; 36:197–199.19. Mouallem M, Friedman E, Shemesh Y, Mayan H, Pauzner R, Farfel Z. Cardiac conduction defects associated with hyponatremia. Clin Cardiol. 1991; 14:165–168.20. Kayal AK, Goswami M, Das M, Jain R. Clinical and biochemical spectrum of hypokalemic paralysis in North: East India. Ann Indian Acad Neurol. 2013; 16:211–217.
