Korean Circ J.
2016 Nov;46(6):791-797. 10.4070/kcj.2016.46.6.791.
The Relationship between Angiotensin-II Type 1 Receptor Gene Polymorphism and Repolarization Parameters after a First Anterior Acute Myocardial Infarction
- Affiliations
-
- 1Department of Public Health and Neurology, Dicle University Medical Faculty, Diyarbakir, Turkey.
- 2Department of Cardiology, Diyarbakır Gazi Yasargil Education and Research Hospital, Diyarbakir, Turkey. droozturk21@hotmail.com
- 3Department of Microbiology, Dicle University Medical Faculty, Diyarbakir, Turkey.
- KMID: 2355454
- DOI: http://doi.org/10.4070/kcj.2016.46.6.791
Abstract
- BACKGROUND AND OBJECTIVES
Genetic influence on T-wave peak to End (Tpe) time in patients with a first anterior acute myocardial infarction (AMI) is uncertain. A polymorphism in the angiotensin-II type 1 receptor (AT1R) gene was discovered recently. The polymorphism consists of an A or C variant, given three different possible genotypes: AA, AC, CC. The purpose of this study was to determine the effects of polymorphism of the AT1R gene polymorphism on Tpe after a first anterior AMI.
SUBJECTS AND METHODS
The subjects were 142 patients (110 men, 32 women, 58±13 years) with a first anterior AMI; ten patients were excluded from this study. Based on the polymorphism of the AT1R gene, they were classified into two groups: Group 1 (AA genotype) of 91 patients and group 2 (AC and CC genotype) of 41 patients. A 12-lead resting ECG was recorded at admission to the coronary care unit in patients with anterior AMI and were manually measured with a ruler. QTc, QTd, QTcd, Tpe, Tpe/QT parameters were measured.
RESULTS
There was no significant difference in the baseline characteristics of patients (p>0.05). We found significant reduction in QTc, QTd, QTcd, Tpe, Tpe/QT indices Group 1 (AA genotype) (mean 66±28 ms) than group 2 (AC and CC genotype) (mean 95±34 ms) (p<0.05).
CONCLUSION
In patients with a first anterior AMI, AT1R gene polymorphisms may influence on repolarization parameters. Although further studies are required.
Figure
-
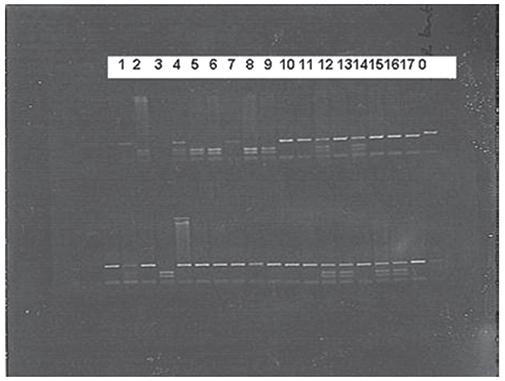
Fig. 1 Gel electrophoresis of the AT1R polymorphism. 0: a DNA size marker (100bp),1: AA, 2: CC, 3: AA, 4: AC, 5: CC, 6: CC, 7: AA, 8: CC, 9: CC, 10: AA, 11: AA, 12: AC, 13: AA, 14: AC, 15: AA, 16: AA, 17: AA.
Reference
-
1. Laragh JH. Renin-angiotensin-aldosterone system for blood pressure and electrolyte homeostasis and its involvement in hypertension, in congestive heart failure and in associated cardiovascular damage (myocardial infarction and stroke). J Hum Hypertens. 1995; 9:385–390.2. Aoki S, Mukae S, Itoh S, et al. The genetic factor in acute myocardial infarction with hypertension. Jpn Circ J. 2001; 65:621–626.3. De Gasparo M, Catt KJ, Inagami T, Wright JW, Unger T. International Union of Pharmacology. XXIII. The angiotensin II receptors. Pharmacol Rev. 2000; 52:415–472.4. Araújo MA, Menezes BS, Lourenço C, Cordeiro ER, Gatti RR, Goulart LR. The A1166C polymorphism of the angiotensin II type-1 receptor in acute myocardial infarction. Arq Bras Cardiol. 2004; 83:409–413.5. Ozturk O, Ozturk U, Bilici A. The effect of angiotensin II type-1 receptor gene polymorphisms on doppler blood flow parameters of carotid and brachial arteries in patients with myocardial infarction. Echocardiography. 2006; 23:536–541.6. Jeron A, Hengstenberg C, Engel S, et al. The D-allele of the ACE polymorphism is related to increased QT dispersion in 609 patients after myocardial infarction. Eur Heart J. 2001; 22:663–668.7. Porthan K, Marjamaa A, Viitasalo M, et al. Relationship of common candidate gene variants to electrocardiographic T-wave peak to T-wave end interval and T-wave morphology parameters. Heart Rhythm. 2010; 7:898–903.8. Anvari A, Türel Z, Schmidt A, et al. Angiotensin converting enzymeand angiotensin II receptor 1polymorphism in coronary disease and malignant ventricular arrhythmias. Cardiovasc Res. 1999; 43:879–883.9. Hamon M, Amant C, Bauters C, et al. Association of angiotensin converting enzyme and angiotensin II type 1 receptor genotypes with left ventricular function and mass in patients with angiographically normal coronary arteries. Heart. 1997; 77:502–505.10. Miller SA, Dykes DD, Polesky HF. Simple salting out procedure for extraction DNA from human nucleoted cells. Nucleic Acids Res. 1988; 16:1215–1219.11. Malik M, Batchvarov VN. Measurement, interpretation and clinical potential of QT dispersion. J Am Coll Cardiol. 2000; 36:1749–1766.12. Lin TH, Chiu HC, Su HM, et al. D-allele of ACE polymorphism is associated with increased magnitude of QT dispersion prolongation in elderly Chinese: 4-year follow-up study. Circ J. 2007; 71:39–45.13. Jeunemaitre X, Ledru F, Battaglia S, et al. Genetic polymorphisms of the renin-angiotensin system and angiographic extent and severity of coronary artery disease: the CORGENE study. Hum Genet. 1997; 99:66–73.14. Eslami V, Safi M, Taherkhani M, Adibi A, Movahed MR. Evaluation of QT, QT dispersion, and T-wave peak to end time changes after primary percutaneous coronaryintervention in patients presenting with acute T-elevation myocardial infarction. J Invasive Cardiol. 2013; 25:232–234.15. Oikarinen L, Nieminen MS, Viitasalo M, et al. Relation of QT interval and QT dispersion to echocardiographic left ventricular hypertrophy and geometric pattern in hypertensive patients: The LIFE study The Losartan Intervention For Endpoint Reduction. J Hypertens. 2001; 19:1883–1891.16. Day CP, McComb JM, Campbell RW. QT dispersion: an indication of arrhythmia risk in patients with long QT intervals. Br Heart J. 1990; 63:342–344.17. Endoh Y, Kasanuki H, Ohnishi S, Uno M. Unsuitability of corrected QT dispersion as a marker for ventricular arrhythmias and cardiac sudden death after acute myocardial infarction. Jpn Circ J. 1999; 63:467–470.18. Fujimoto S, Uemura S, Tomoda Y, et al. Effects of exercise training on the heart rate variability and QT dispersion of patients with acute myocardial infarction. Jpn Circ J. 1999; 63:577–582.19. Takezako T, Zhang B, Serikawa T, Fan P, Nomoto J, Saku K. The D allele of the angiotensin-converting enzyme gene and reperfusioninduced ventricular arrhythmias in patients with acute myocardial infarction. Jpn Circ J. 2001; 65:603–609.20. Gubaev KI, Nasibullin TR, Zakirova AN, Mustafina OE. Association of polymorphic markers I/D of gene ACE and A1166C of gene AT2R1 with ischemic chronic heart failure in the Russian and Tatar populations of Bashkortostan Republic. Genetika. 2006; 42:1712–1717.21. Jin Y, Kuznetsova T, Thijs L, et al. Association of left ventricular mass with the AGTR1 A1166C polymorphism. Am J Hypertens. 2012; 25:472–478.22. De Sutter J, Tavernier R, Van De Wiele C, et al. QT dispersion is not related to infarct size or inducibility in patients with coronary artery disease and life threatening ventricular arrhythmias. Heart. 1999; 81:533–538.23. Blanco RR, Austin H, Vest RN, et al. Angiotensin receptor type 1 single nucleotide polymorphism 1166A/C is associated with malignant arrhythmias and altered circulating miR-155 levels in patients with chronic heart failure. J Card Fail. 2012; 18:717–723.24. Miller JA, Thai K, Scholey JW. Angiotensin II type 1 receptor gene polymorphism predicts response to losartan and angiotensin II. Kidney Int. 1999; 56:2173–2180.25. Spargias KS, Lindsay SJ, Hall AS, Cowan JC, Ball SG. Ramipril reduces QT dispersion in patients with acute myocardial infarction and heart failure. Am J Cardiol. 1999; 83:969–971.26. Karpanou EA, Vyssoulis GP, Psichogios A, et al. Regression of left ventricular hypertrophy results in improvement of QT dispersion in patients with hypertension. Am Heart J. 1998; 136:765–768.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Association Analysis of a Polymorphism of the Angiotensin I-Converting Enzyme Gene and Angiotensin II Type 1 Receptor Gene in Korean Population
- Angiotensin-converting enzyme gene polymorphism is not associated with myocardial infarction in Koreans
- Dispersion of QT Interval and Other Repolarization Indexes in Acute Myocardial Infarction
- An I/D Polymorphism in Angiotensin-Converting Enzyme Gene in Myocardial Infarction
- Relationship between Angiotensin I Converting Enzyme Gene Polymorphism and Vascular complications in Non-Insulin Dependent Diabetic Patients
