Abductor Reconstruction with Gluteus Maximus Transfer in Primary Abductor Deficiency during Total Hip Arthroplasty
- Affiliations
-
- 1Department of Orthopaedic Surgery, Daegu Fatima Hospital, Daegu, Korea. femur1973@gmail.com
- KMID: 2354551
- DOI: http://doi.org/10.5371/hp.2016.28.3.178
Abstract
- Abductor deficiency in native hip joint may cause severe limping and pain. It is more serious situation in case of arthroplasty due to instability and recurrent dislocation. Well-known causes of abductor deficiency are repeated surgery, chronic trochanteric bursitis, superior gluteal nerve injury, failure of repair of abductor tendon insertion to the greater trochanter. Author had experienced primary abductor deficiency during total hip replacement and treated successfully with the transfer of gluteus maximus. We'd like to introduce the operation technique with the review of literature.
Keyword
Figure
-

Fig. 1 Preoperative anteroposterior pelvis radiographs shows osteoarthritis of left hip joint following dysplasia.
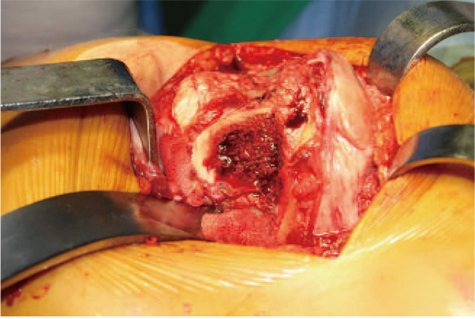
Fig. 2 No muscle attachment but only fascia attachment at the tip of the greater trochanter is shown.
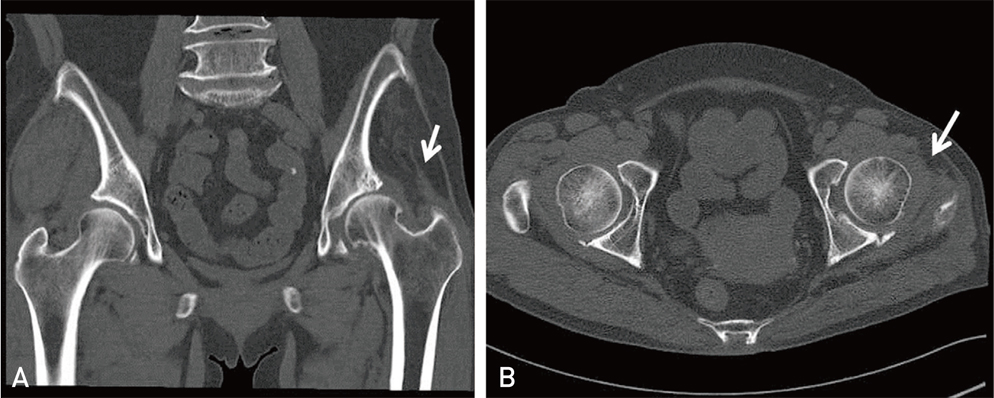
Fig. 3 White arrow indicates (A) fatty change of glumeus medius and minimus and (B) tensor fascia latae in preoperative computed tomography scan.
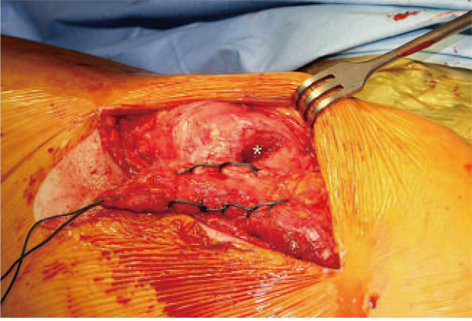
Fig. 4 It shows harvested muscle of anterior fiber of gluteus maximus and bone tunnel (asterisk) at the greater trochanter.

Fig. 5 Intraoperative photographs. (A) The harvested muscle was passed through the bone tunnel from medial to lateral aspect. (B) Non-absorable suture material was passed through the hole made by kirschner wire crossing the proximal femur. (C) The harvested muscle passed through the bone tunnel is securely sutured.
Reference
-
1. Gottschalk F, Kourosh S, Leveau B. The functional anatomy of tensor fasciae latae and gluteus medius and minimus. J Anat. 1989; 166:179–189.2. Davies H, Zhaeetan S, Tavakkolizadeh A, Janes G. Surgical repair of chronic tears of the hip abductor mechanism. Hip Int. 2009; 19:372–376.
Article3. Bird PA, Oakley SP, Shnier R, Kirkham BW. Prospective evaluation of magnetic resonance imaging and physical examination findings in patients with greater trochanteric pain syndrome. Arthritis Rheum. 2001; 44:2138–2145.
Article4. Baker AS, Bitounis VC. Abductor function after total hip replacement. An electromyographic and clinical review. J Bone Joint Surg Br. 1989; 71:47–50.
Article5. Daly PJ, Morrey BF. Operative correction of an unstable total hip arthroplasty. J Bone Joint Surg Am. 1992; 74:1334–1343.
Article6. Fehm MN, Huddleston JI, Burke DW, Geller JA, Malchau H. Repair of a deficient abductor mechanism with Achilles tendon allograft after total hip replacement. J Bone Joint Surg Am. 2010; 92:2305–2311.
Article7. Kohl S, Evangelopoulos DS, Siebenrock KA, Beck M. Hip abductor defect repair by means of a vastus lateralis muscle shift. J Arthroplasty. 2012; 27:625–629.
Article8. Whiteside LA. Surgical technique: Transfer of the anterior portion of the gluteus maximus muscle for abductor deficiency of the hip. Clin Orthop Relat Res. 2012; 470:503–510.
Article9. Whiteside LA. Surgical technique: Gluteus maximus and tensor fascia lata transfer for primary deficiency of the abductors of the hip. Clin Orthop Relat Res. 2014; 472:645–653.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Total Hip Replacement Arthroplasty for the Old Dislocated Hip
- Extension Contracture of Both Hip Joints Secondary to Congenital Fibrous Bands of Both Gluteus Maximus Muscles: Case Report
- Gluteus Maximus Fibrosis: Report of 3 Cases
- Comparisons of Test-Retest Reliability of Strength Measurement of Gluteus Medius Strength between Break and Make Test in Subjects with Pelvic Drop
- Contracture of the Hip Secondary to Fibrosis of the Gluteus Maximus Muscle
