Feasibility of transanal endoscopic total mesorectal excision for rectal cancer: results of a pilot study
- Affiliations
-
- 1Center for Colorectal Cancer, Research Institute and Hospital, National Cancer Center, Goyang, Korea. gsgabal@ncc.re.kr
- KMID: 2354326
- DOI: http://doi.org/10.4174/astr.2016.91.4.187
Abstract
- PURPOSE
To evaluate the feasibility of transanal total mesorectal excision (TME) in patients with rectal cancer.
METHODS
This study enrolled 12 patients with clinically node negative rectal cancer located 4-12 cm from the anal verge who underwent transanal endoscopic TME with the assistance of single port laparoscopic surgery between September 2013 and August 2014. The primary endpoint was TME quality; secondary endpoints included number of harvested lymph nodes and postoperative complications within 30 days (NCT01938027).
RESULTS
The 12 patients included 7 males and 5 females, of median age 59 years and median body mass index 24.2 kg/m². Tumors were located on average 6.7 cm from the anal verge. Four patients (33.3%) received preoperative chemoradiotherapy. Median operating time was 195 minutes and median blood loss was 50 mL. There were no intraoperative complications and no conversions to open surgery. TME was complete or nearly complete in 11 patients (91.7%). Median distal resection and circumferential resection margins were 18.5 mm and 10 mm, respectively. Median number of harvested lymph nodes was 15. Median length of hospital stay was 9 days. There were no postoperative deaths. Six patients experienced minor postoperative complications, including urinary dysfunction in 2, transient ileus in 3, and wound abscess in 1.
CONCLUSION
This pilot study showed that high-quality TME was possible in most patients without serious complications. Transanal TME for patients with rectal cancer may be feasible and safe, but further investigations are necessary to evaluate its long-term functional and oncologic outcomes and to clarify its indications.
Keyword
MeSH Terms
-
Abscess
Body Mass Index
Chemoradiotherapy
Female
Humans
Ileus
Intraoperative Complications
Laparoscopy
Length of Stay
Lymph Nodes
Male
Minimally Invasive Surgical Procedures
Natural Orifice Endoscopic Surgery
Pilot Projects*
Postoperative Complications
Rectal Neoplasms*
Transanal Endoscopic Surgery
Wounds and Injuries
Figure
-
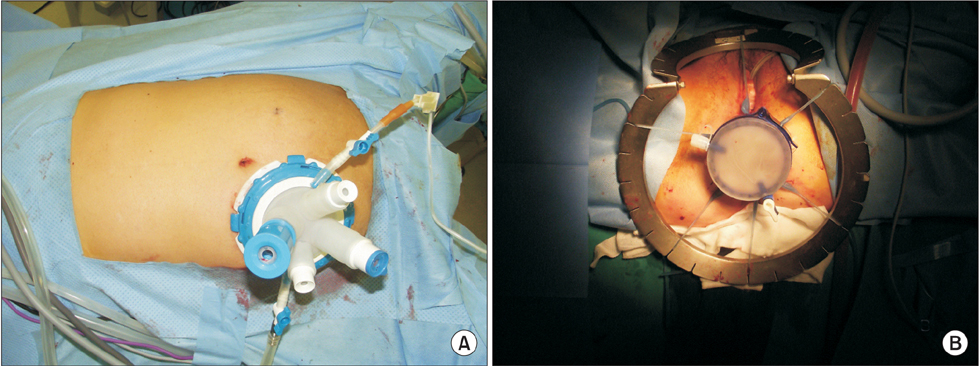
Fig. 1 Illustration of the procedure. (A) An Octoport (Dalim, Seoul, Korea) was placed on the potential ileostomy site of the right iliac fossa. (B) A GelPOINT path (Applied Medical Inc., Rancho Santa Margarita, CA, USA) was installed at the anus after purse string suturing and full-thickness circumferential transection of the distal part of the tumor.
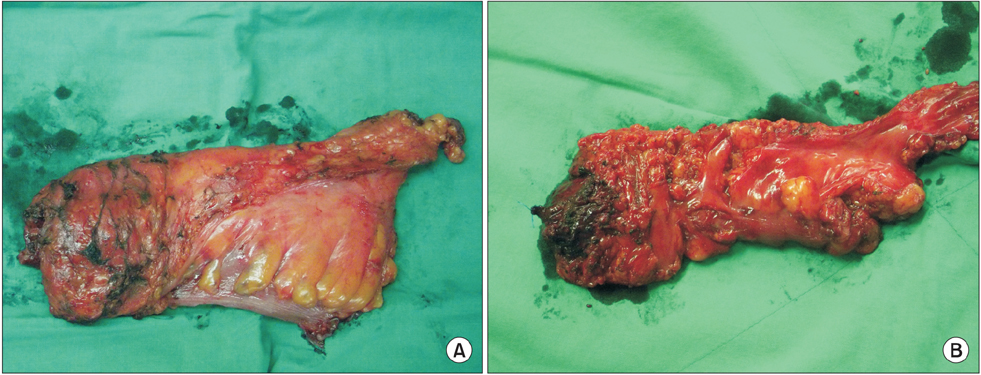
Fig. 2 Grading of surgical specimens. (A) The specimen removed from patient No. 1 was graded as 'complete' total mesorectal excision (TME) according to the Quirke method. (B) Due to the quality of the mesorectum, the specimen removed from patient No. 2 was graded as 'incomplete' TME.
Cited by 1 articles
-
Feasibility of transanal total mesorectal excision in cases with challenging patient and tumor characteristics
Dae Kyung Sohn, Sung Chan Park, Min Jung Kim, Hee Jin Chang, Kyung Su Han, Jae Hwan Oh
Ann Surg Treat Res. 2019;96(3):123-130. doi: 10.4174/astr.2019.96.3.123.
Reference
-
1. Martling AL, Holm T, Rutqvist LE, Moran BJ, Heald RJ, Cedemark B. Effect of a surgical training programme on outcome of rectal cancer in the County of Stockholm. Stockholm Colorectal Cancer Study Group, Basingstoke Bowel Cancer Research Project. Lancet. 2000; 356:93–96.2. Guillou PJ, Quirke P, Thorpe H, Walker J, Jayne DG, Smith AM, et al. Short-term endpoints of conventional versus laparoscopic-assisted surgery in patients with colorectal cancer (MRC CLASICC trial): multicentre, randomised controlled trial. Lancet. 2005; 365:1718–1726.3. van der Pas MH, Haglind E, Cuesta MA, Fürst A, Lacy AM, Hop WC, et al. Laparoscopic versus open surgery for rectal cancer (COLOR II): short-term outcomes of a randomised, phase 3 trial. Lancet Oncol. 2013; 14:210–218.4. Jeong SY, Park JW, Nam BH, Kim S, Kang SB, Lim SB, et al. Open versus laparoscopic surgery for mid-rectal or low-rectal cancer after neoadjuvant chemoradiotherapy (COREAN trial): survival outcomes of an open-label, non-inferiority, randomised controlled trial. Lancet Oncol. 2014; 15:767–774.5. Atallah S, Martin-Perez B, Albert M, deBeche-Adams T, Nassif G, Hunter L, et al. Transanal minimally invasive surgery for total mesorectal excision (TAMISTME): results and experience with the first 20 patients undergoing curativeintent rectal cancer surgery at a single institution. Tech Coloproctol. 2014; 18:473–480.6. Sylla P, Rattner DW, Delgado S, Lacy AM. NOTES transanal rectal cancer resection using transanal endoscopic microsurgery and laparoscopic assistance. Surg Endosc. 2010; 24:1205–1210.7. Velthuis S, Nieuwenhuis DH, Ruijter TE, Cuesta MA, Bonjer HJ, Sietses C. Transanal versus traditional laparoscopic total mesorectal excision for rectal carcinoma. Surg Endosc. 2014; 28:3494–3499.8. de Lacy AM, Rattner DW, Adelsdorfer C, Tasende MM, Fernández M, Delgado S, et al. Transanal natural orifice transluminal endoscopic surgery (NOTES) rectal resection: "down-to-up" total mesorectal excision (TME): short-term outcomes in the first 20 cases. Surg Endosc. 2013; 27:3165–3172.9. Tuech JJ, K aroui M, Lelong B, De Chaisemartin C, Bridoux V, Manceau G, et al. A step toward NOTES total mesorectal excision for rectal cancer: endoscopic transanal proctectomy. Ann Surg. 2015; 261:228–233.10. Rouanet P, Mourregot A, Azar CC, Carrere S, Gutowski M, Quenet F, et al. Transanal endoscopic proctectomy: an innovative procedure for difficult resection of rectal tumors in men with narrow pelvis. Dis Colon Rectum. 2013; 56:408–415.11. Marks J, Nassif G, Schoonyoung H, DeNittis A, Zeger E, Mohiuddin M, et al. Sphincter-sparing surgery for adenocarcinoma of the distal 3 cm of the true rectum: results after neoadjuvant therapy and minimally invasive radical surgery or local excision. Surg Endosc. 2013; 27:4469–4477.12. Jorge JM, Wexner SD. Etiology and management of fecal incontinence. Dis Colon Rectum. 1993; 36:77–97.13. Quirke P, Durdey P, Dixon MF, Williams NS. Local recurrence of rectal adenocarcinoma due to inadequate surgical resection. Histopathological study of lateral tumour spread and surgical excision. Lancet. 1986; 2:996–999.14. Glynne-Jones R, Mawdsley S, Novell JR. The clinical significance of the circumferential resection margin following preoperative pelvic chemo-radiotherapy in rectal cancer: why we need a common language. Colorectal Dis. 2006; 8:800–807.15. Knol JJ, D'Hondt M, Souverijns G, Heald B, Vangertruyden G. Transanal endoscopic total mesorectal excision: technical aspects of approaching the mesorectal plane from below: a preliminary report. Tech Coloproctol. 2015; 19:221–229.16. Whiteford MH, Denk PM, Swanström LL. Feasibility of radical sigmoid colectomy performed as natural orifice translumenal endoscopic surgery (NOTES) using transanal endoscopic microsurgery. Surg Endosc. 2007; 21:1870–1874.17. Sylla P, Sohn DK, Cizginer S, Konuk Y, Turner BG, Gee DW, et al. Survival study of natural orifice translumenal endoscopic surgery for rectosigmoid resection using transanal endoscopic microsurgery with or without transgastric endoscopic assistance in a swine model. Surg Endosc. 2010; 24:2022–2030.18. Sohn DK, Jeong SY, Park JW, Kim JS, Hwang JH, Kim DW, et al. Comparative study of NOTES rectosigmoidectomy in a swine model: E-NOTES vs. P-NOTES. Endoscopy. 2011; 43:526–532.19. Telem DA, Han KS, Kim MC, Ajari I, Sohn DK, Woods K, et al. Transanal rectosigmoid resection via natural orifice translumenal endoscopic surgery (NOTES) with total mesorectal excision in a large human cadaver series. Surg Endosc. 2013; 27:74–80.20. Leroy J, Cahill RA, Peretta S, Marescaux J. Single port sigmoidectomy in an experimental model with survival. Surg Innov. 2008; 15:260–265.21. Park YM, Cho E, Kang HY, Kim JM. The effectiveness and safety of endoscopic submucosal dissection compared with endoscopic mucosal resection for early gastric cancer: a systematic review and metaanalysis. Surg Endosc. 2011; 25:2666–2677.22. Fernandez-Hevia M, Delgado S, Castells A, Tasende M, Momblan D, Díaz del Gobbo G, et al. Transanal total mesorectal excision in rectal cancer: short-term outcomes in comparison with laparoscopic surgery. Ann Surg. 2015; 261:221–227.23. Emhoff IA, Lee GC, Sylla P. Transanal colorectal resection using natural orifice translumenal endoscopic surgery (NOTES). Dig Endosc. 2014; 26:Suppl 1. 29–42.24. Nagtegaal ID, Marijnen CA, Kranenbarg EK, van de Velde CJ, van Krieken JH, et al. Pathology Review Committee. Circumferential margin involvement is still an important predictor of local recurrence in rectal carcinoma: not one millimeter but two millimeters is the limit. Am J Surg Pathol. 2002; 26:350–357.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Surgical Techniques for Transanal Local Excision for Early Rectal Cancer
- Feasibility of transanal total mesorectal excision in cases with challenging patient and tumor characteristics
- Transanal total mesorectal excision for rectal cancer: it’s come a long way and here to stay
- Transanal Total Mesorectal Excision for Rectal Cancer: Perioperative and Oncological Outcomes
- Transanal Endoscopic and Transabdominal Robotic Total Mesorectal Excision for Mid-to-Low Rectal Cancer: Comparison of Short-term Postoperative and Oncologic Outcomes by Using a Case-Matched Analysis
