Clin Exp Otorhinolaryngol.
2016 Sep;9(3):206-211. 10.21053/ceo.2015.01116.
Audiologic Patterns of Otic Capsule Preserving Temporal Bone Fracture: Effects of the Affected Subsites
- Affiliations
-
- 1Department of Otorhinolaryngology, Boramae Medical Center, Seoul Metropolitan Government-Seoul National University, Seoul, Korea.
- KMID: 2353617
- DOI: http://doi.org/10.21053/ceo.2015.01116
Abstract
OBJECTIVES
This study was aimed to assess the relationship between the type of temporal bone area involved and conductive hearing loss.
METHODS
We enrolled 97 patients who visited the otolaryngology clinics of Seoul National University Hospital or Boramae Medical Center, Seoul Metropolitan Government-Seoul National University with temporal bone fracture between January 2004 and January 2014. Audiometric parameters, including initial and improved air-bone (AB) conduction gap values, were reviewed in accordance with the temporal bone computed tomography (external auditory canal [EAC], middle ear [ME], mastoid [M], and ossicle [O]).
RESULTS
Patients with ossicular chain involvement exhibited a larger AB gap compared to those with no ossicular chain involvement at 250, 1,000, 2,000, and 4,000 Hz. Among the groups without ossicular chain involvement, the initial AB gap was largest in patients with EAC+ME+M involvement, followed by the ME+M and M-only involvement groups. The greatest improvement in the AB gap was observed in the EAC+ME+M group followed by the ME+M and M-only groups, irrespective of ossicular chain involvement. Improvements in AB gap values were smallest at 2,000 Hz.
CONCLUSION
Conductive hearing loss pattern differed according to the temporal bone area involved. Therefore, areas such as the hematoma and hemotympanum, as well as the fracture line of the temporal bone area, must be evaluated to predict audiologic patterns with otic capsule preserving temporal bone fracture.
Keyword
MeSH Terms
Figure
-
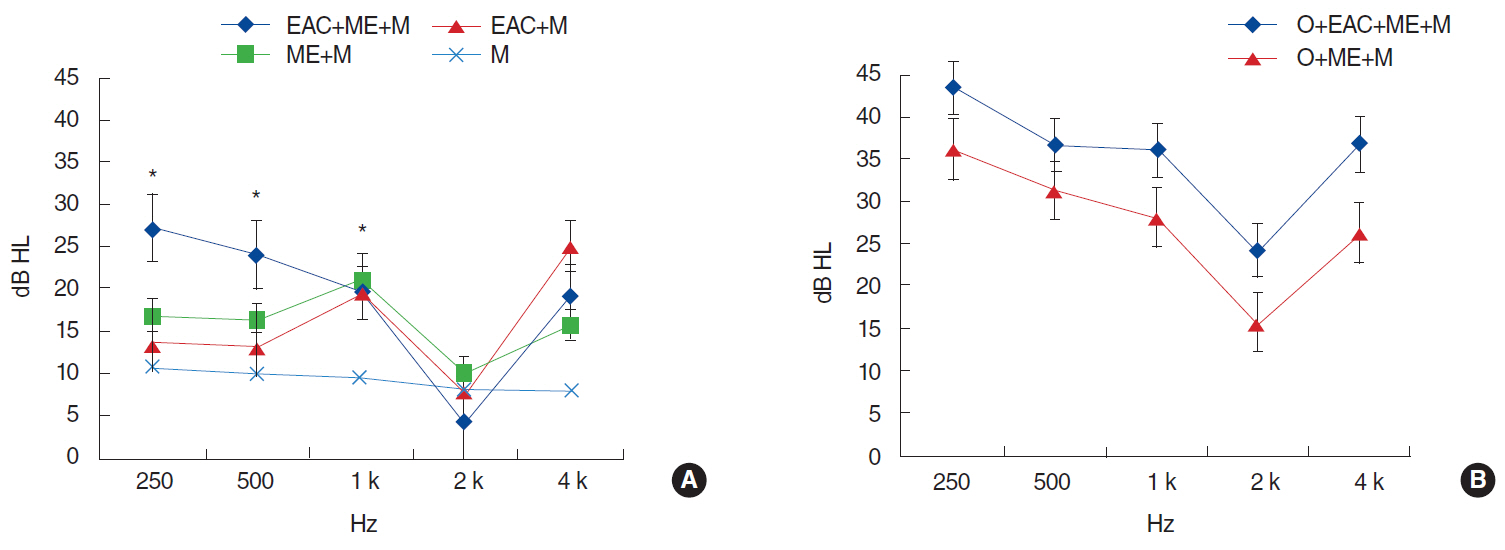
Fig. 1. Initial air-bone gap according to involvement range of temporal bone. (A) Patients with intact ossicular chain. (B) Patients with ossicular chain disruption or dislocation. EAC, external auditory canal; ME, middle ear; M, mastoid; O, ossicle. *P<0.05.
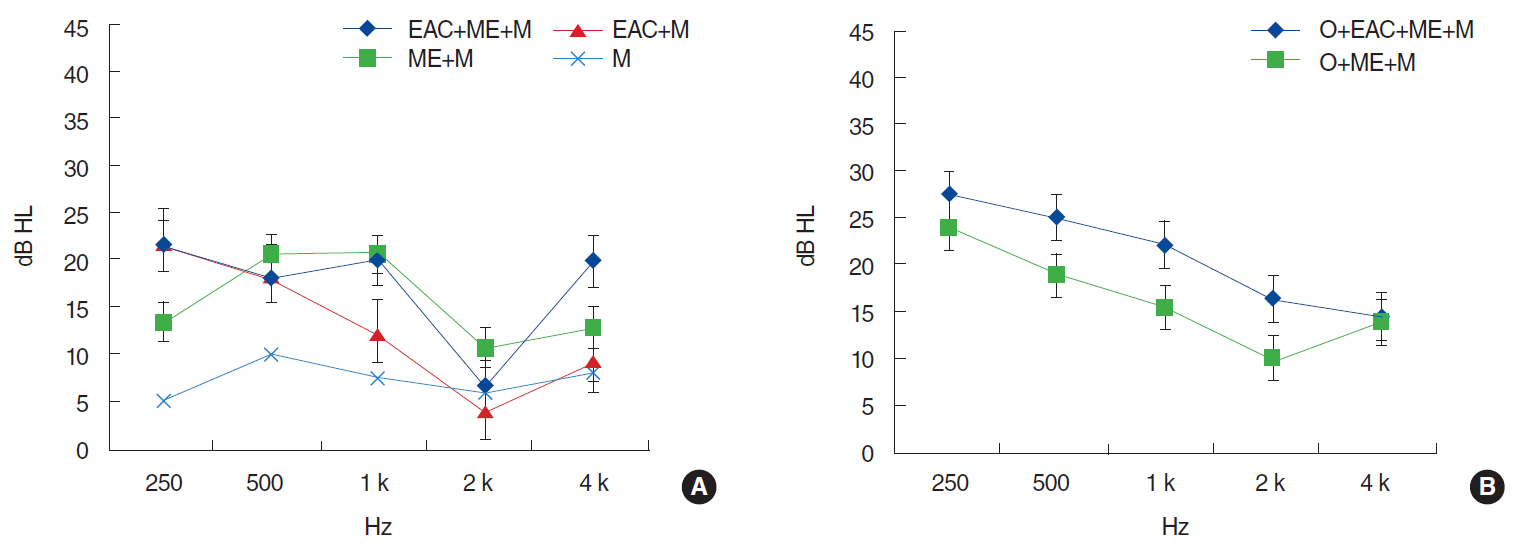
Fig. 2. Improvement of air-bone gap (initial air-bone gap – final air-bone gap) according to involvement range of temporal bone. (A) Patients with intact ossicular chain. (B) Patients with ossicular chain disruption or dislocation. EAC, external auditory canal; ME, middle ear; M, mastoid; O, ossicle. *P<0.05.
Reference
-
1. Johnson F, Semaan MT, Megerian CA. Temporal bone fracture: evaluation and management in the modern era. Otolaryngol Clin North Am. 2008; Jun. 41(3):597–618.
Article2. Nicol JW, Johnstone AJ. Temporal bone fractures in children: a review of 34 cases. J Accid Emerg Med. 1994; Dec. 11(4):218–22.
Article3. Wysocki J. Cadaveric dissections based on observations of injuries to the temporal bone structures following head trauma. Skull Base. 2005; May. 15(2):99–106.
Article4. Ishman SL, Friedland DR. Temporal bone fractures: traditional classification and clinical relevance. Laryngoscope. 2004; Oct. 114(10):1734–41.
Article5. Dahiya R, Keller JD, Litofsky NS, Bankey PE, Bonassar LJ, Megerian CA. Temporal bone fractures: otic capsule sparing versus otic capsule violating clinical and radiographic considerations. J Trauma. 1999; Dec. 47(6):1079–83.
Article6. Kang HM, Kim MG, Boo SH, Kim KH, Yeo EK, Lee SK, et al. Comparison of the clinical relevance of traditional and new classification systems of temporal bone fractures. Eur Arch Otorhinolaryngol. 2012; Aug. 269(8):1893–9.
Article7. Little SC, Kesser BW. Radiographic classification of temporal bone fractures: clinical predictability using a new system. Arch Otolaryngol Head Neck Surg. 2006; Dec. 132(12):1300–4.8. Rafferty MA, Mc Conn Walsh R, Walsh MA. A comparison of temporal bone fracture classification systems. Clin Otolaryngol. 2006; Aug. 31(4):287–91.
Article9. Sun GH, Shoman NM, Samy RN, Cornelius RS, Koch BL, Pensak ML. Do contemporary temporal bone fracture classification systems reflect concurrent intracranial and cervical spine injuries? Laryngoscope. 2011; May. 121(5):929–32.
Article10. Montava M, Mancini J, Masson C, Collin M, Chaumoitre K, Lavieille JP. Temporal bone fractures: sequelae and their impact on quality of life. Am J Otolaryngol. 2015; May-Jun. 36(3):364–70.
Article11. Yetiser S, Hidir Y, Gonul E. Facial nerve problems and hearing loss in patients with temporal bone fractures: demographic data. J Trauma. 2008; Dec. 65(6):1314–20.
Article12. Blake DM, Tomovic S, Jyung RW. Temporal bone fracture. Ear Nose Throat J. 2014; Jan. 93(1):16–25.
Article13. Ravicz ME, Rosowski JJ, Merchant SN. Mechanisms of hearing loss resulting from middle-ear fluid. Hear Res. 2004; Sep. 195(1-2):103–30.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Utility of Brain Computed Tomography in Detecting Fractures of the Temporal Bones Correlated with Patterns of Fracture on High-Resolution Computed Tomography
- Clinical Study on the Reliable Temporal Bone Fracture Classification Scheme
- A Case of Cochlear Implantation after Bilateral Temporal Bone Fracture
- Pneumolabyrinth Associated with Otic Capsule-Violating Fracture: Diagnosis and Clinical Features
- Temporal Bone Fracture and Labyrinthine Concussion as Ataxic Gait in 21-Months-Old Child
