Surgical Outcome of Minimal Resection with Full Thickness Rotating Suture Technique for Lower Lid Epiblepharon
- Affiliations
-
- 1Department of Ophthalmology, Dong-A University College of Medicine, Busan, Korea. hbahn@dau.ac.kr
- KMID: 2351863
- DOI: http://doi.org/10.3341/jkos.2016.57.9.1348
Abstract
- PURPOSE
To introduce the minimal skin and orbicularis oculi muscle resection with the full thickness rotating suture technique for lower lid epiblepharon and to assess its surgical outcome.
METHODS
A retrospective review of medical records was performed on lower lid epiblepharon patients who were followed for more than 6 months after surgical correction performed between January 2004 and December 2015. All surgeries were performed by one surgeon using minimal skin and orbicularis oculi muscle resection and the full thickness rotating suture technique for lower lid epiblepharon correction.
RESULTS
A total of 943 lower lid epiblepharon patients (403 male, 540 female) were included in the analysis. The mean patient age was 6.7 ± 2.4 years, and the mean postoperative follow-up was 12.9 ± 7.2 months. Eyelid shape and function were well maintained in 904 patients (95.9%), with no recurrence during follow-up. Among the recurrent cases (39 patients [4.1%]), 19 patients (2%) underwent a second correction surgery.
CONCLUSIONS
Minimal skin and orbicularis oculi muscle resection with the full thickness rotating suture technique for lower lid epiblepharon showed good surgical outcome with few complications and high success rate.
MeSH Terms
Figure
-
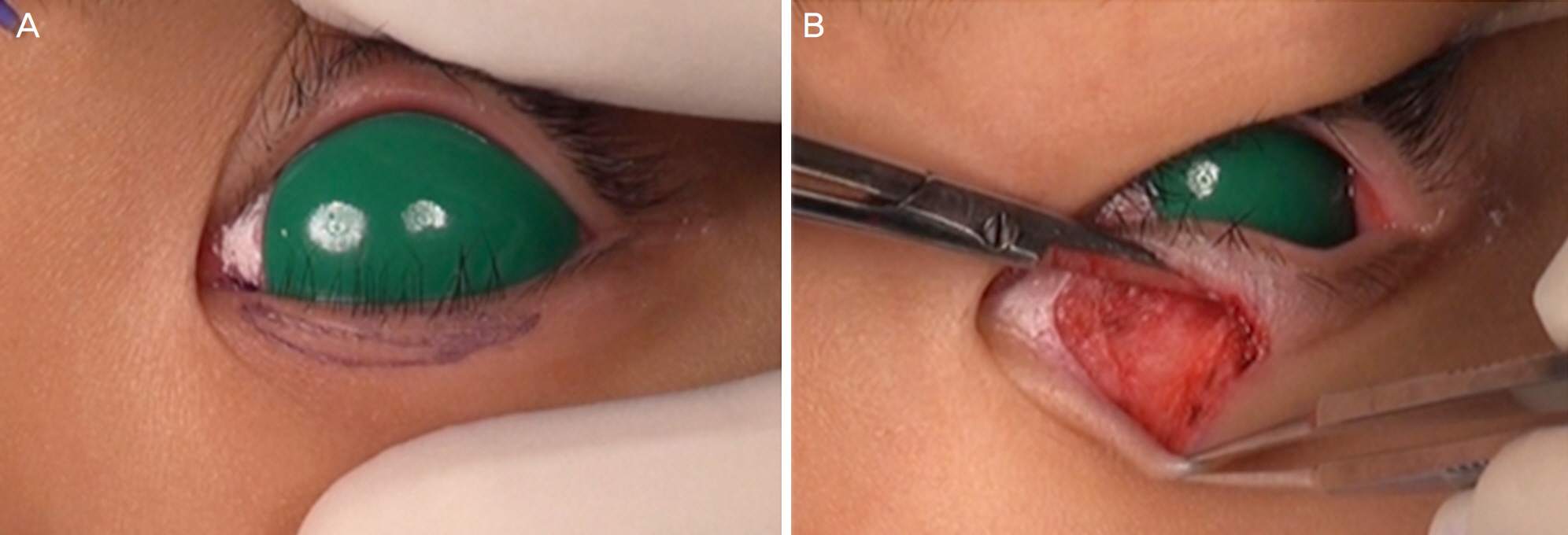
Figure 1. Minimal resection of skin & orbicularis oculi muscle. Marking a skin incision line with the aid of Bishop forceps (medial side is wide and tapered laterally, like tadpole shape) (A). Skin and subcutaneous tissue resection was performed with Stevens scissors (B).

Figure 2. Photography describing full thickness rotating suture. After exposing the tarsal plate, simple interrupted buried suture is performed (A, B). Cross section view of the lower eyelid with full thickness rotating suture (C).
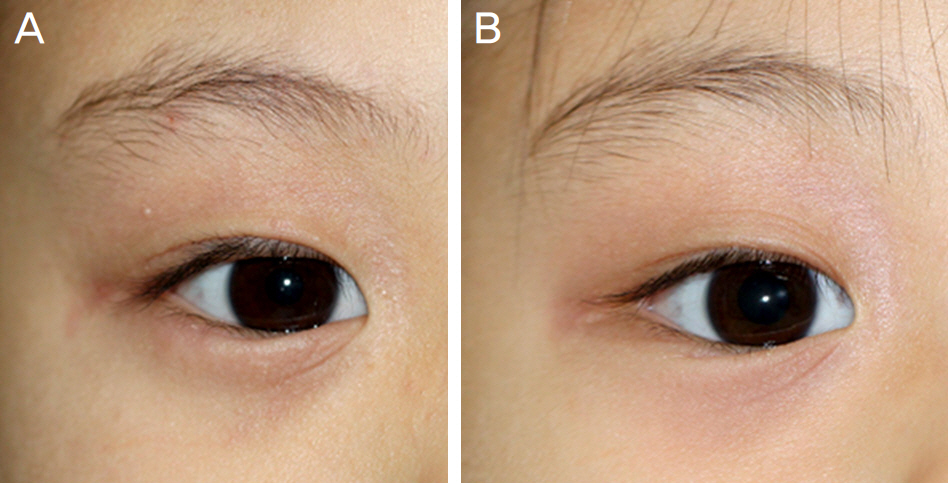
Figure 3. Photography showing preoperative & postoperative view. Preoperative view (A). Postoperative 6 month view (B). Lower eyelid margin is well everted and the cornea is not touched by cilia anymore.
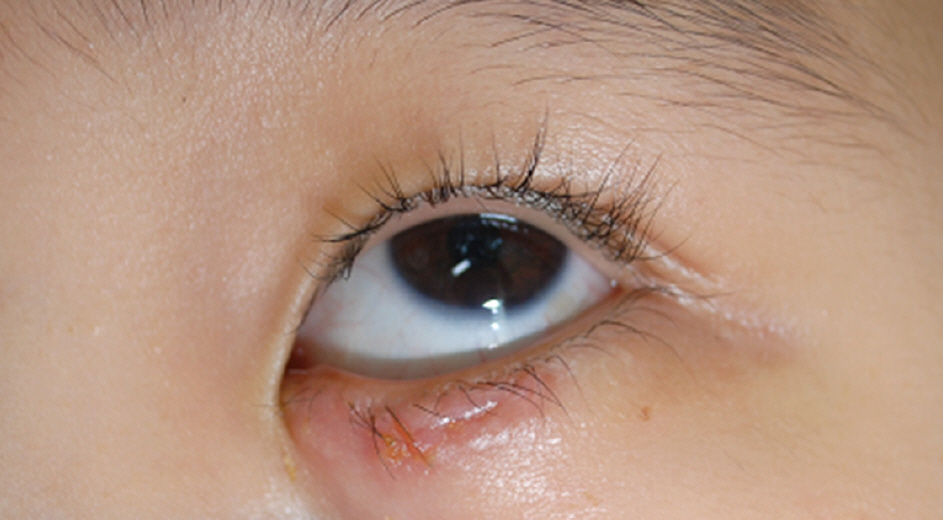
Figure 4. Photography showing hypertrophic scar at post-operative 3 months. The scar was formed along the skin incision line which creates mechanical tension.
Reference
-
References
1. Levitt JM. Epiblepharon and congenital entropion. Am J Ophthalmol. 1957; 44:112–3.
Article2. Johnson CC. Epiblepharon. Am J Ophthalmol. 1968; 66:1172–5.
Article3. Johnson CC. Epicanthus and epiblepharon. Arch Ophthalmol. 1978; 96:1030–3.
Article4. Karlin DB. Congeital entropion, epiblepharon, and antimongoloid obiliquity of the palperbral fissure. Am J Ophthalmol. 1960; 50:487–93.5. Quickert MH, Wilkes DI, Dryden RM. Nonincisional correction of epiblepharon and congenital entropion. Arch Ophthalmol. 1983; 101:778–81.
Article6. Millman AL, Mannor GF, Putterman AM. Lid crease and capsu-lopalpebral fascia repair in congenital entropion and epiblepharon. Ophthalmic Surg. 1994; 25:162–5.
Article7. Kim JS, Jin SW, Hur MC, et al. The clinical characteristics and abdominal outcomes of epiblepharon in Korean children: a 9-year experience. J Ophthalmol. 2014; 2014:156501.8. Hotz FC. A new operation for entropion and trichiasis. Arch Ophthalmol. 1879; 8:249–63.9. Hotz FC. Remarks on 177 operations for entropion and trichiasis. Arch Ophthalmol. 1882; 11:442–50.10. Woo KI, Yi K, Kim YD. Surgical correction for lower lid epiblepharon in Asians. Br J Ophthalmol. 2000; 84:1407–10.
Article11. Yi K, Ku HJ, Kim TW, Kim YD. Surgical correction fo epiblepharon. J Korean Ophthalmol Soc. 1998; 39:11–6.12. Noda S, Hayasaka S, Setogawa T. Epiblepharon with inverted eyelashes in Japanese children. I. Incidence and symptoms. Br J Ophthalmol. 1989; 73:126–7.
Article13. Hwang JM, Lee JH. Clinical evaluation of epiblepharon. J Korean Ophthalmol Soc. 1988; 29:1–5.14. Hayasaka S, Noda S, Setogawa T. Epiblepharon with inverted eyelashes in Japanese children. Ⅱ. Surgical repairs. Br J Ophthalmol. 1989; 73:128–30.15. Kim SY, Moon IA, Kang YK, Yang SW. Clinical evaluation of epiblepharon and congenital entropion. J Korean Ophthalmol Soc. 1999; 40:646–51.16. Sohn SW, Woo KI, Chang HR. Astigmatism in children with epiblepharon. J Korean Ophthalmol Soc. 2002; 43:1827–32.17. Sundar G, Young SM, Tara S, et al. Epiblepharon in East Asian abdominals: the Singapore experience. Ophthalmology. 2010; 117:184–9.18. Choo C. Correction of oriental epiblepharon by anterior lamellar reposition. Eye (Lond). 1996; 10(Pt 5):545–7.
Article19. Kim MS, Sa HS, Lee JY. Surgical correction of epiblepharon using an epicanthal weakening procedure with lash rotating sutures. Br J Ophthalmol. 2014; 98:120–3.
Article20. Khwarg SI, Choung HK. Epiblepharon of the lower eyelid: technique of surgical repair and quantification of excision according to the skin fold height. Ophthalmic Surg Lasers. 2002; 33:280–7.
Article21. Ni J, Shao C, Wang K, et al. Modified Hotz procedure combined with modified Z-epicanthoplasty versus modified Hotz procedure alone for epiblepharon repair. Ophthal Plast Reconstr Surg. 2016 Mar 4. [Epub ahead of print].
Article22. Fujiwara T, Maeda M, Kuwae K, Nishino K. Modified split V-W plasty for entropion with an epicanthal fold in Asian eyelids. Plast Reconstr Surg. 2006; 118:635–42.
Article23. Asamura S, Nakao H, Kakizaki H, Isogai N. Is it truly necessary to add epicanthoplasty for correction of the epiblepharon? J Craniofac Surg. 2013; 24:1137–40.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Results of the Celsus-Hotz Procedure and Rotating Suture Technique in the Surgical Correction of the Epiblepharon
- Modified Continuous Buried Suture Technique for Upper Lid Epiblepharon
- The Surgical Effect of Full-Thickness Eyelid Resection in Traumatic Blepharoptosis
- Surgical Correction of Congenital Epiblepharon: Lower Eyelid Crease Reforming Technique
- 3-year Outcomes of Rotating Suture with Root Z-epicanthoplasty for Lower Lid Epiblepharon
