Comparison of Endovascular Treatments of Ruptured Dissecting Aneurysms of the Intracranial Internal Carotid Artery and Vertebral Artery with a Review of the Literature
- Affiliations
-
- 1Department of Neurosurgery, Seoul National University Bundang Hospital, Seongnam, Korea.
- 2Department of Neurosurgery, Hanyang University Medical Center, Seoul, Korea. hjyi8499@hanyang.ac.kr
- KMID: 2351712
- DOI: http://doi.org/10.3340/jkns.2016.59.5.449
Abstract
OBJECTIVE
Subarachnoid hemorrhage (SAH) caused by rupture of an internal carotid artery (ICA) or vertebral artery (VA) dissecting aneuryesm is rare. Various treatment strategies have been used for ruptured intracranial dissections. The purpose of this study is to compare the clinical and angiographic characteristics and outcomes of endovascular treatment for ruptured dissecting aneurysms of the intracranial ICA and VA.
METHODS
The authors retrospectively reviewed a series of patients with SAH caused by ruptured intracranial ICA and VA dissecting aneurysms from March 2009 to April 2014. The relevant demographic and angiographic data were collected, categorized and analyzed with respect to the outcome.
RESULTS
Fifteen patients were identified (6 ICAs and 9 VAs). The percentage of patients showing unfavorable initial clinical condition and a history of hypertension was higher in the VA group. The initial aneurysm detection rate and the percentage of fusiform aneurysms were higher in the VA group. In the ICA group, all patients were treated with double stent-assisted coiling, and showed favorable outcomes. In the VA group, 2 patients were treated with double stent-assisted coiling and 7 with endovascular trapping. Two patients died and 1 patient developed severe disability.
CONCLUSION
Clinically, grave initial clinical condition and hypertension were more frequent in the VA group. Angiographically, bleb-like aneurysms were more frequent in the ICA group and fusiform aneurysms were more frequent in the VA group. Endovascular treatment of these aneurysms is feasible and the result is acceptable in most instances.
Keyword
MeSH Terms
Figure
-
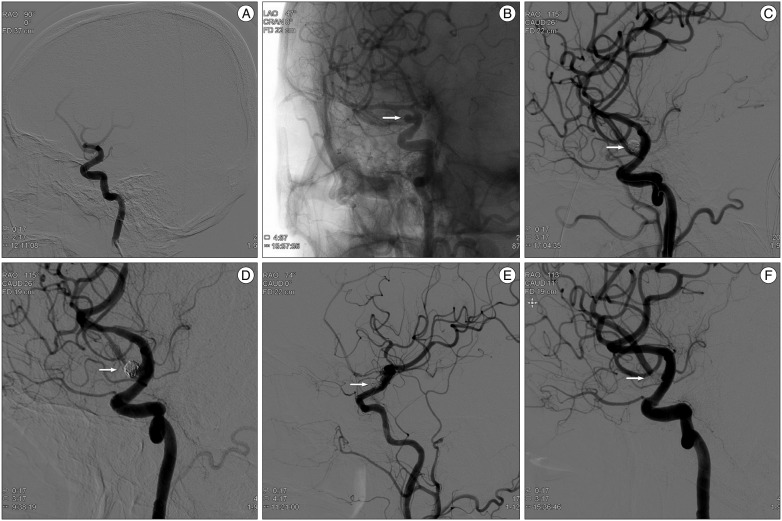
Fig. 1 ICA Case 3. A 54-year-old woman, Hunt and Hess grade 3, presented with Fisher grade 4 SAH. A : Femoral angiogram demonstrates suspicious outpouching on the right supraclinoid carotid artery. B : Angiogram after 7 days revealed saccular outgrowth indicating dissecting aneurysm (white arrow). C : Stent-assisted coiling was performed (Enterprise 4.5/28 mm) with resultant near complete occlusion without contrast leakage (white arrow). D : Follow-up angiography after 2 weeks revealed regrowth of aneurysmal sac. Additional stent-assisted coiling (Enterprise 4.5/28) was performed (white arrow). E : Final angiogram showed near complete occlusion of the aneurysm (white arrow). F : After 6 months, follow-up angiogram showed no evidence of aneurysmal regrowth (white arrow). ICA : internal carotid artery, SAH : subarachnoid hemorrhage.
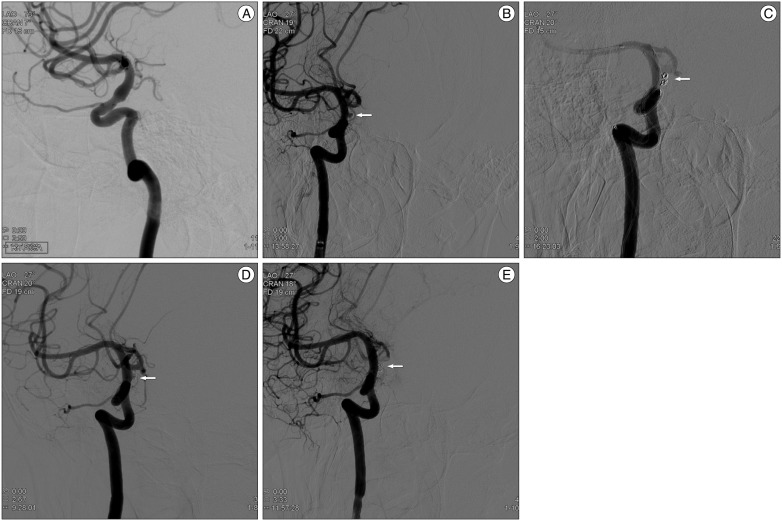
Fig. 2 ICA Case 5. A 39-year-old man, Hunt and Hess grade 2, was presented with Fisher grade 2 SAH. A : Angiogram revealed unremarkable results similar to CT angiogram. He was admitted to the intensive care unit for close observation. B : On the 5th hospital day, angiogram revealed a bleb-like dissecting aneurysm (white arrow) on the right distal carotid artery. C : Double stent-assisted coiling was performed (Enterprise 4.5/22, 4.5/28 mm), and control angiogram showed incomplete occlusion of the dissecting aneurysm (white arrow). D : Follow-up angiogram after 2 weeks failed to show any change in the lesion (white arrow). E : Follow-up angiogram after 6 months revealed further thrombosis within the aneurysm (white arrow). ICA : internal carotid artery, SAH : subarachnoid hemorrhage.
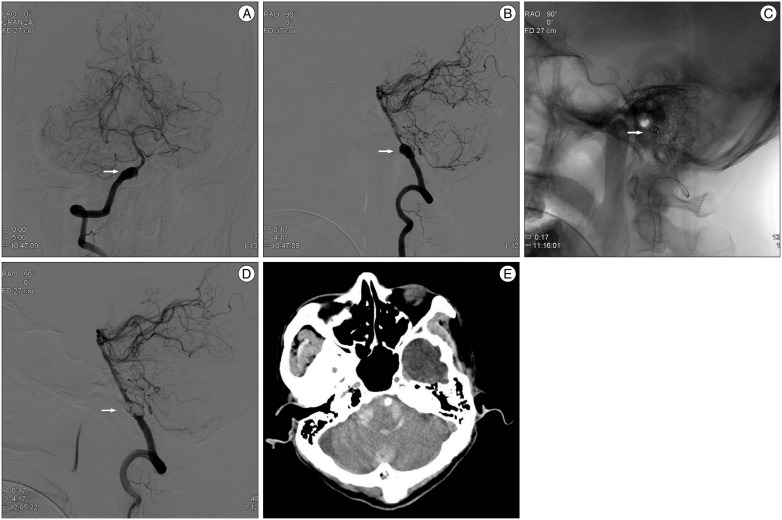
Fig. 3 VA Case 7. A 52-year-old man, Hunt and Hess grade 1, was presented with Fisher grade 4 SAH. A and B : Angiogram demonstrated a definite dissecting aneurysm (white arrow) on the right VA traversing the right posterior inferior cerebellar artery (PICA). Right VA was the dominant vessel, and the dissecting aneurysm incorporated the origin of the right PICA. C : Double stent insertion was performed (Enterprise, 4.5/28, 4.5/37 mm), and then, 14 coils were then placed in the aneurysmal sac with jailing technique (white arrow). D : Final angiogram showed partial occlusion of the aneurysm, but without any contrast leakage. He improved gradually until the 14th hospital day (white arrow). E : Brain CT showed dense infratentorial SAH and intraventricular hemorrhage in the 4th ventricle. He remained unconsciousless for a few days until demise. VA : vertebral artery, SAH : subarachnoid hemorrhage.
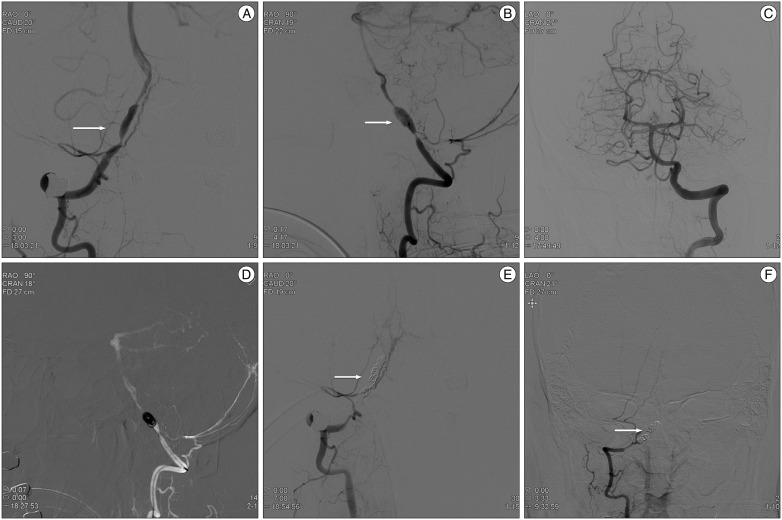
Fig. 4 VA Case 12. A 52-year-old man, Hunt and Hess grade 3, was presented with Fisher grade 4 SAH. A and B : Angiogram demonstrated a typical pearl and string dissection (white arrow) in the right VA incorporating the right PICA. C : Left VA was the dominant vessel, and the dissecting aneurysm in the right VA incorporated the origin of the right PICA. However, the inferior territory of the cerebellum was perfused by the right anterior inferior cerebellar artery and the left PICA. D : Right VA was sacrificed with trapping with coiling. E : Final angiogram showed complete occlusion of the aneurysm and inferior cerebellar perfusion was intact (white arrow). F : After 6 months, follow-up angiogram showed no evidence of recanalization or aneurysmal regrowth (white arrow). VA : vertebral artery, SAH : subarachnoid hemorrhage, PICA : posterior inferior cerebellar artery.
Cited by 1 articles
-
Does Neurosurgical Clipping or Endovascular Coiling Lead to More Cases of Delayed Hydrocephalus in Patients with Subarachnoid Hemorrhage?
Tae Oong Eom, Eun Suk Park, Jun Bum Park, Soon Chan Kwon, Hong Bo Sim, In Uk Lyo, Min Soo Kim
J Cerebrovasc Endovasc Neurosurg. 2018;20(2):87-95. doi: 10.7461/jcen.2018.20.2.87.
Reference
-
1. Ahn JY, Chung SS, Lee BH, Kim SH, Yoon PH, Joo JY, et al. Treatment of spontaneous arterial dissections with stent placement for preservation of the parent artery. Acta Neurochir (Wien). 2005; 147:265–273. discussion 273PMID: 15625588.
Article2. Ahn JY, Han IB, Kim TG, Yoon PH, Lee YJ, Lee BH, et al. Endovascular treatment of intracranial vertebral artery dissections with stent placement or stent-assisted coiling. AJNR Am J Neuroradiol. 2006; 27:1514–1520. PMID: 16908571.3. Albuquerque FC, Fiorella DJ, Han PP, Deshmukh VR, Kim LJ, McDougall CG. Endovascular management of intracranial vertebral artery dissecting aneurysms. Neurosurg Focus. 2005; 18:E3. PMID: 15715448.
Article4. Anxionnat R, de Melo Neto JF, Bracard S, Lacour JC, Pinelli C, Civit T, et al. Treatment of hemorrhagic intracranial dissections. Neurosurgery. 2003; 53:289–300. discussion 300-301PMID: 12925243.
Article5. Fischer S, Perez MA, Kurre W, Albes G, Bäzner H, Henkes H. Pipeline embolization device for the treatment of intra- and extracranial fusiform and dissecting aneurysms : initial experience and long-term follow-up. Neurosurgery. 2014; 75:364–374. discussion 374. PMID: 24871140.
Article6. Gonzalez AM, Narata AP, Yilmaz H, Bijlenga P, Radovanovic I, Schaller K, et al. Blood blister-like aneurysms : single center experience and systematic literature review. Eur J Radiol. 2014; 83:197–205. PMID: 24231267.
Article7. Hamada J, Kai Y, Morioka M, Yano S, Todaka T, Ushio Y. Multimodal treatment of ruptured dissecting aneurysms of the vertebral artery during the acute stage. J Neurosurg. 2003; 99:960–966. PMID: 14705721.
Article8. Kashiwazaki D, Ushikoshi S, Asano T, Kuroda S, Houkin K. Long-term clinical and radiological results of endovascular internal trapping in vertebral artery dissection. Neuroradiology. 2013; 55:201–206. PMID: 23149552.
Article9. Kim BC, Kwon OK, Oh CW, Bang JS, Hwang G, Jin SC, et al. Endovascular internal carotid artery trapping for ruptured blood blister-like aneurysms : long-term results from a single centre. Neuroradiology. 2014; 56:211–217. PMID: 24430115.
Article10. Kim BM, Shin YS, Kim SH, Suh SH, Ihn YK, Kim DI, et al. Incidence and risk factors of recurrence after endovascular treatment of intracranial vertebrobasilar dissecting aneurysms. Stroke. 2011; 42:2425–2430. PMID: 21778439.
Article11. Kitanaka C, Sasaki T, Eguchi T, Teraoka A, Nakane M, Hoya K. Intracranial vertebral artery dissections : clinical, radiological features, and surgical considerations. Neurosurgery. 1994; 34:620–626. discussion 626-627PMID: 8008158.12. Kocaeli H, Chaalala C, Andaluz N, Zuccarello M. Spontaneous intradural vertebral artery dissection : a single-center experience and review of the literature. Skull Base. 2009; 19:209–218. PMID: 19881901.
Article13. Kurata A, Ohmomo T, Miyasaka Y, Fujii K, Kan S, Kitahara T. Coil embolization for the treatment of ruptured dissecting vertebral aneurysms. AJNR Am J Neuroradiol. 2001; 22:11–18. PMID: 11158881.14. Lee BH, Kim BM, Park MS, Park SI, Chung EC, Suh SH, et al. Reconstructive endovascular treatment of ruptured blood blister-like aneurysms of the internal carotid artery. J Neurosurg. 2009; 110:431–436. PMID: 19046039.
Article15. Meckel S, Singh TP, Undrén P, Ramgren B, Nilsson OG, Phatouros C, et al. Endovascular treatment using predominantly stent-assisted coil embolization and antiplatelet and anticoagulation management of ruptured blood blister-like aneurysms. AJNR Am J Neuroradiol. 2011; 32:764–771. PMID: 21372169.
Article16. Meling TR, Sorteberg A, Bakke SJ, Slettebø H, Hernesniemi J, Sorteberg W. Blood blister-like aneurysms of the internal carotid artery trunk causing subarachnoid hemorrhage : treatment and outcome. J Neurosurg. 2008; 108:662–671. PMID: 18377243.
Article17. Mizutani T. Subarachnoid hemorrhage associated with angiographic "stenotic" or "occlusive" lesions in the carotid circulation. Surg Neurol. 1998; 49:495–503. discussion 503-504PMID: 9586926.
Article18. Mizutani T, Aruga T, Kirino T, Miki Y, Saito I, Tsuchida T. Recurrent subarachnoid hemorrhage from untreated ruptured vertebrobasilar dissecting aneurysms. Neurosurgery. 1995; 36:905–911. discussion 912-913PMID: 7791980.
Article19. Mohammadian R, Taheraghdam AA, Sharifipour E, Mansourizadeh R, Pashapour A, Shimia M, et al. Endovascular treatment of intracranial artery dissection : clinical and angiographic follow-up. Neurol Res Int. 2013; 2013:968380. PMID: 23970969.20. Nakatomi H, Nagata K, Kawamoto S, Shiokawa Y. Ruptured dissecting aneurysm as a cause of subarachnoid hemorrhage of unverified etiology. Stroke. 1997; 28:1278–1282. PMID: 9183362.
Article21. Ohkuma H, Nakano T, Manabe H, Suzuki S. Subarachnoid hemorrhage caused by a dissecting aneurysm of the internal carotid artery. J Neurosurg. 2002; 97:576–583. PMID: 12296641.
Article22. Rabinov JD, Hellinger FR, Morris PP, Ogilvy CS, Putman CM. Endovascular management of vertebrobasilar dissecting aneurysms. AJNR Am J Neuroradiol. 2003; 24:1421–1428. PMID: 12917140.23. Sakata N, Takebayashi S, Kojima M, Masawa N, Suzuki K, Takatama M. Pathology of a dissecting intracranial aneurysm. Neuropathology. 2000; 20:104–108. PMID: 10935447.
Article24. Sim SY, Chung J, Shin YS. Are blood blister-like aneurysms a specific type of dissection? A comparative study of blood blister-like aneurysms and ruptured mizutani type 4 vertebral artery dissections. J Korean Neurosurg Soc. 2014; 56:395–399. PMID: 25535516.
Article25. Sugiu K, Tokunaga K, Watanabe K, Sasahara W, Ono S, Tamiya T, et al. Emergent endovascular treatment of ruptured vertebral artery dissecting aneurysms. Neuroradiology. 2005; 47:158–164. PMID: 15703929.
Article26. Taha MM, Sakaida H, Asakura F, Maeda M, Toma N, Yamamoto A, et al. Endovascular management of vertebral artery dissecting aneurysms : review of 25 patients. Turk Neurosurg. 2010; 20:126–135. PMID: 20401839.27. Takemoto K, Abe H, Uda K, Inoue T. Surgical treatment of intracranial VA dissecting aneurysm. Acta Neurochir Suppl. 2010; 107:51–56. PMID: 19953371.
Article28. Uhl E, Schmid-Elsaesser R, Steiger HJ. Ruptured intracranial dissecting aneurysms : management considerations with a focus on surgical and endovascular techniques to preserve arterial continuity. Acta Neurochir (Wien). 2003; 145:1073–1083. discussion 1083-1084PMID: 14663564.29. van Oel LI, van Rooij WJ, Sluzewski M, Beute GN, Lohle PN, Peluso JP. Reconstructive endovascular treatment of fusiform and dissecting basilar trunk aneurysms with flow diverters, stents, and coils. AJNR Am J Neuroradiol. 2013; 34:589–595. PMID: 22918431.
Article30. Yamada M, Kitahara T, Kurata A, Fujii K, Miyasaka Y. Intracranial vertebral artery dissection with subarachnoid hemorrhage : clinical characteristics and outcomes in conservatively treated patients. J Neurosurg. 2004; 101:25–30. PMID: 15255247.
Article31. Yamaura A, Watanabe Y, Saeki N. Dissecting aneurysms of the intracranial vertebral artery. J Neurosurg. 1990; 72:183–188. PMID: 2404089.
Article32. Yonekawa Y, Zumofen D, Imhof HG, Roth P, Khan N. Hemorrhagic cerebral dissecting aneurysms : surgical treatments and results. Acta Neurochir Suppl. 2008; 103:61–69. PMID: 18496947.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Stent-Assisted Coil Trapping in a Manual Internal Carotid Artery Compression Test for the Treatment of a Fusiform Dissecting Aneurysm
- Endovascular Treatments for Ruptured Intracranial Vertebral Artery Dissecting Aneurysms: Experience in 16 Patients
- Early Rebleeding after Internal Trapping of a Ruptured Vertebral Artery Dissecting Aneurysm: A Case Report
- Endovascular Coil Trapping of a Ruptured Dissecting Aneurysm of the Vertebral Artery Using Detachable Coils and Micro-Tornado(R) Coils
- Endovascular Treatment of Ruptured Dissecting Aneurysms on the P2-3 Segment of the Posterior Cerebral Artery: A Report of Two Cases
