Celiac axis stenosis as a rare but critical condition treated with pancreatoduodenectomy: report of 2 cases
- Affiliations
-
- 1Center for Liver Cancer, National Cancer Center, Goyang, Korea. lsd@ncc.re.kr
- KMID: 2350543
- DOI: http://doi.org/10.4174/astr.2016.91.3.149
Abstract
- We describe 2 cases of patients with loss of hepatic arterial flow during surgery for pancreatic head cancer due to celiac stenosis caused by median arcuate ligament compression. The first case underwent pylorus-resecting pancreatoduodenectomy for pancreatic head cancer. After resection of the gastroduodenal artery, flow in the common hepatic artery disappeared, and celiac axis stenosis was identified. Interventional stent insertion was attempted, however, it failed due to the acute angle of the celiac orifice (os). This problem was resolved by arterial reconstruction. The second case underwent pylorus-preserving pancreatoduodenectomy for pancreatic head cancer and the same phenomenon occurred during the procedure. Interventional stent insertion was also tried; in this patient, however, it failed due to the acute angle of the celiac os. The problem was resolved by changing a femoral approach to a brachial approach, and the stent was inserted into the celiac os successfully.
MeSH Terms
Figure
-
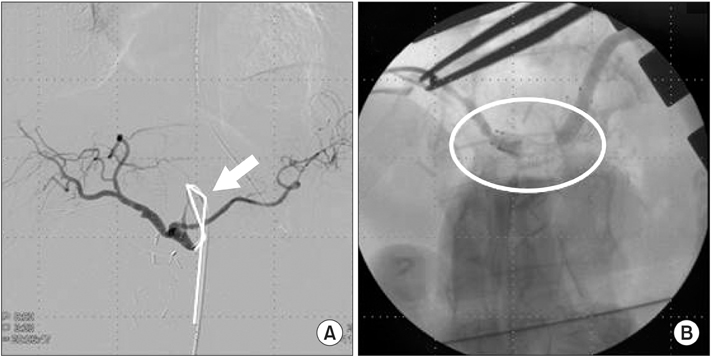
Fig. 1 A 57-year-old female who received pylorus-resecting PD for pancreatic head cancer, after the resection of gastroduodenal artery (GDA); the flow of common hepatic artery was not detected and celiac axis stenosis was identified intraoperatively. (A) Intervention failed due to acute angulation (full line, arrow) of the celiac orifice. (B) The patient was sent back to operating room, and stent insertion (circle) was performed through GDA stump intraoperatively.
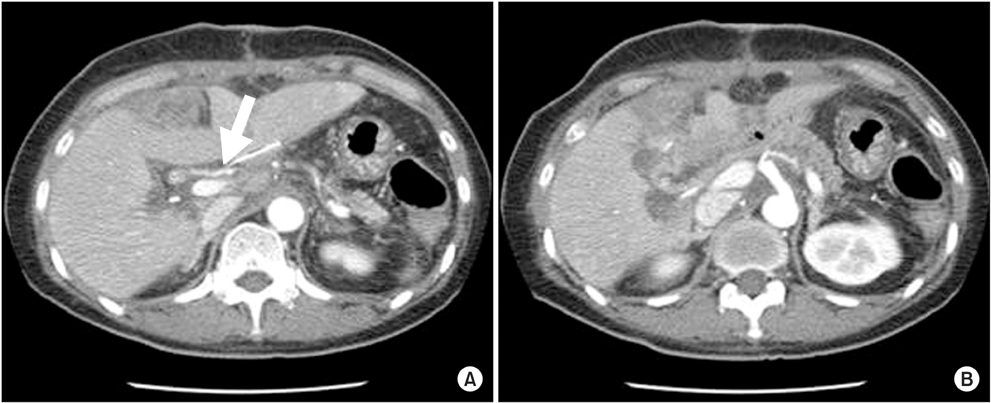
Fig. 2 Postoperative CT image of 1st case. (A) Patent arterial flow of common hepatic artery (arrow) and intrahepatic arteries. (B) Stent located at celiac orifice and showed patent arterial flow to the splenic artery.
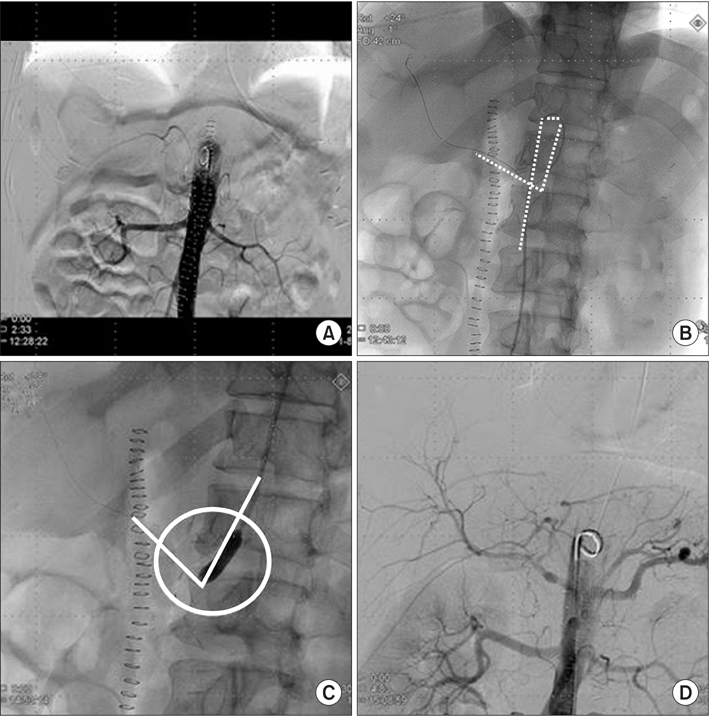
Fig. 3 A 56-year-old male received pylorus-preserving PD for pancreatic head cancer, and loss of hepatic artery flow was detected after gastroduodenal artery ligation. (A) On abdominal arteriography, the flow to the celiac trunk was delayed severely. (B) Approach of the balloon and stent was impossible due to acute angulation (dotted line) of the celiac orifice. (C) Ballooning and stent insertion for stenotic lesion (circle) by the brachial approach (full line) was performed. (D) Arterial flow was improved after the procedure.
Reference
-
1. Bron KM, Redman HC. Splanchnic artery stenosis and occlusion. Incidence; arteriographic and clinical manifestations. Radiology. 1969; 92:323–328.2. Szilagyi DE, Rian RL, Elliott JP, Smith RF. The celiac artery compression syndrome: does it exist? Surgery. 1972; 72:849–863.3. Nara S, Sakamoto Y, Shimada K, Sano T, Kosuge T, Takahashi Y, et al. Arterial reconstruction during pancreatoduodenectomy in patients with celiac axis stenosis: utility of Doppler ultrasonography. World J Surg. 2005; 29:885–889.4. Park CM, Chung JW, Kim HB, Shin SJ, Park JH. Celiac axis stenosis: incidence and etiologies in asymptomatic individuals. Korean J Radiol. 2001; 2:8–13.5. Berney T, Pretre R, Chassot G, Morel P. The role of revascularization in celiac occlusion and pancreatoduodenectomy. Am J Surg. 1998; 176:352–356.6. Sugae T, Fujii T, Kodera Y, Kanzaki A, Yamamura K, Yamada S, et al. Classification of the celiac axis stenosis owing to median arcuate ligament compression, based on severity of the stenosis with subsequent proposals for management during pancreatoduodenectomy. Surgery. 2012; 151:543–549.7. Turner KM, Majekodunmi K, Manejwala A, Neschis D, Novak Z, Boutros C. Image findings in celiac artery stenosis due to median arcuate ligament compression: a crucial diagnosis when planning for pancreaticoduodenectomy. J Gastrointest Surg. 2014; 18:638–640.8. Farma JM, Hoffman JP. Nonneoplastic celiac axis occlusion in patients undergoing pancreaticoduodenectomy. Am J Surg. 2007; 193:341–344.9. Horton KM, Talamini MA, Fishman EK. Median arcuate ligament syndrome: evaluation with CT angiography. Radiographics. 2005; 25:1177–1182.10. Sharafuddin MJ, Olson CH, Sun S, Kresowik TF, Corson JD. Endovascular treatment of celiac and mesenteric arteries stenoses: applications and results. J Vasc Surg. 2003; 38:692–698.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Celiac Axis Stenosis: Incidence and Etiologies in Asymptomatic Individuals
- Embolization of Inferior Pancreaticoduodenal Artery Aneurysm with Celiac Stenosis or Occlusion: A Report of Three Cases and a Review of Literature
- Duplex Ultrasonography in the Detection of Celiac Axis Stenosis: A Validation Study
- Open surgical decompression of celiac axis compression by division of the median arcuate ligament
- A Dissecting Aneurysm of the Common and Proper Hepatic Artery with Dissection of the Celiac Axis and the SMA
