MRI Findings of Intrinsic and Extrinsic Duodenal Abnormalities and Variations
- Affiliations
-
- 1Department of Radiology, Ankara University School of Medicine, Ankara 06100, Turkey. ebrumd2001@yahoo.com
- 2Department of Gastroenterology, Ankara University School of Medicine, Ankara 06100, Turkey.
- KMID: 2344277
- DOI: http://doi.org/10.3348/kjr.2015.16.6.1240
Abstract
- This pictorial review aims to illustrate the magnetic resonance imaging (MRI) findings and presentation patterns of anatomical variations and various benign and malignant pathologies of the duodenum, including sphincter contraction, major papilla variation, prominent papilla, diverticulum, annular pancreas, duplication cysts, choledochocele, duodenal wall thickening secondary to acute pancreatitis, postbulbar stenosis, celiac disease, fistula, choledochoduodenostomy, external compression, polyps, Peutz-Jeghers syndrome, ampullary carcinoma and adenocarcinoma. MRI is a useful imaging tool for demonstrating duodenal pathology and its anatomic relationships with adjacent organs, which is critical for establishing correct diagnosis and planning appropriate treatment, especially for surgery.
Keyword
MeSH Terms
-
Ampulla of Vater/anatomy & histology/radiography
Choledochal Cyst/pathology/radiography
Diverticulum/radiography
Duodenal Diseases/pathology/*radiography
Duodenum/*anatomy & histology/radiography
Humans
*Magnetic Resonance Imaging
Pancreas/abnormalities/anatomy & histology/radiography
Pancreatic Diseases/radiography
Figure
-
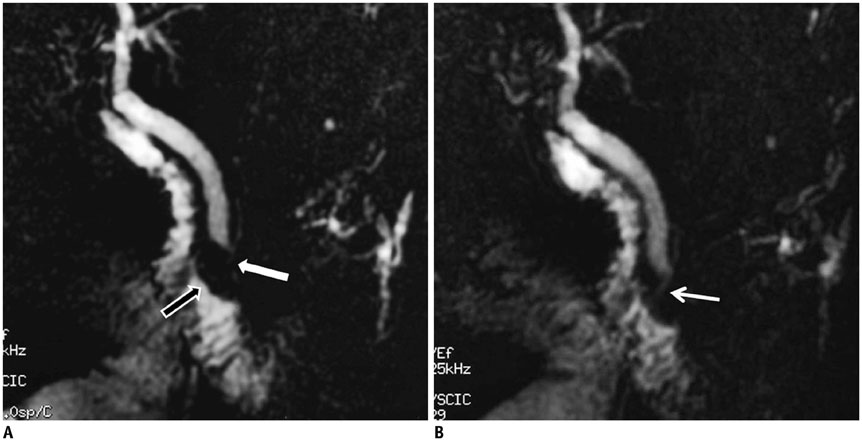
Fig. 1 Physiological sphincter contraction. On this MRCP image, major papilla (black arrow) appears very prominent at medial part of second section of duodenum (A). Distal choledochus is not visible (white arrow). Only after some relaxation of sphincter of Oddi did intramural segment of choledochus (arrow) become apparent (B). This image represents normal sphincter contractility. In order for morphologic changes and contractility in Vaterian sphincter complex to be evaluated optimally, they must be visualized both during contraction and during maximum relaxation. For this reason, it is necessary for patient to hold his or her breath in order to obtain serial MRCP images. MRCP = magnetic resonance cholangiopancreatography
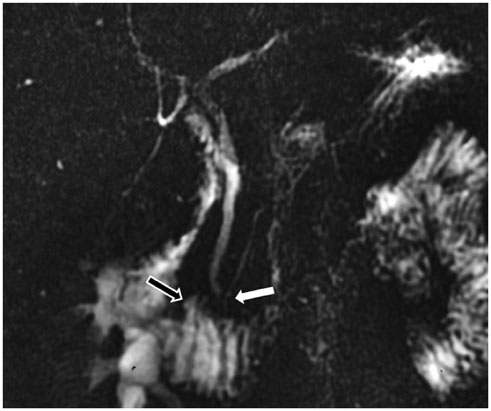
Fig. 2 Opening of distal end of choledochus to 3rd segment of duodenum. On this MRCP image, small periampullary diverticulum is depicted (black arrow), and also in this patient, major papilla variationally opens to 3rd section of duodenum (white arrow). Major papilla is in horizontal, i.e., 3rd, segment at rate of 25%. MRCP = magnetic resonance cholangiopancreatography

Fig. 3 Prominent papilla. On coronal fast imaging employing steady-state acquisition MR image, nodular structure (arrow) is detected at level of major papilla (hypertrophic papilla). Normally, papilla is scarcely distinguished from surrounding duodenal mucosal folds, but as seen in this image, normal papillas may be seen as oval protruding structures of 5-10 mm. MRI and magnetic resonance cholangiopancreatography are important in hypertrophic papilla diagnosis and in detecting underlying pathology.

Fig. 4 Diverticulum. Diverticulum appears as fluid-filled pouch that protrudes from lumen of 3rd section of duodenum on this magnetic resonance cholangiopancreatography image (arrow). Diverticula are frequent in duodenum, and they are most often encountered in medial wall of 2nd and 3rd duodenal segments.

Fig. 5 Diverticulum. On MRCP, large diverticulum located distally in 3rd segment of duodenum is seen (arrow). If diverticula appear completely in fluid signal, they may misdiagnosed as cystic tumors of pancreas on CT or MRI. MRCP is highly successful both in imaging biliary tree and in determining liquid structures and their origins in this localization. MRCP = magnetic resonance cholangiopancreatography

Fig. 6 Diverticulum. On axial T2-weighted (A) and magnetic resonance cholangiopancreatography (B) images, 4 cm diverticulum (white arrows in A) is seen at transverse segment of duodenum. On axial section (A), air within diverticulum lumen causes signal void (arrowheads in A). In addition, choledochus (arrow in B) is larger than expected, with filling defects within its lumen related to stones and stent (B). Air-fluid level within diverticulum is important sign that allows its recognition on axial sections and also allows differentiation from other cystic lesions that may be encountered within region. D = diverticulum
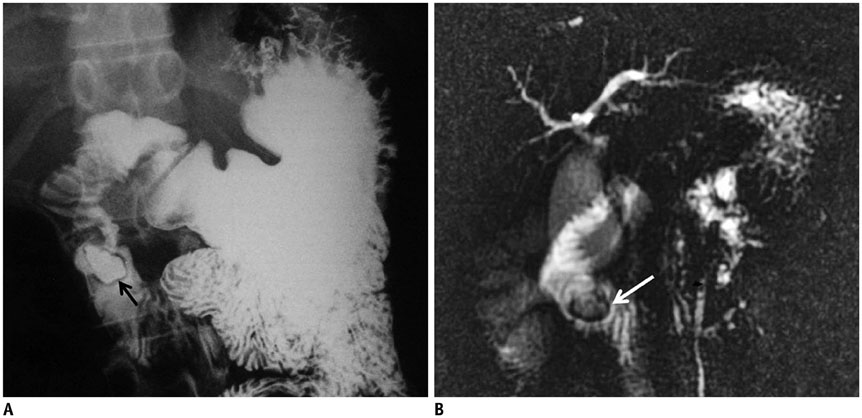
Fig. 7 Intraluminal duodenal diverticulum (IDD) in patient with anal atresia corrected by surgery. In barium study, contrast-filled inpouching towards lumen (arrow) is detected at 2nd portion of duodenum with radiolucent rim (halo sign) (A). In same patient, magnetic resonance cholangiopancreatography (MRCP) image shows fluid collection surrounded by hypointense rim (arrow) in duodenal lumen (B). Intraluminal fluid collection on T2-weighted image with hypointense rim that changes shape with peristaltism on MRCP is almost characteristic sign for IDD. By means of multiplanar imaging, it is possible to view diverticulum wall in duodenum lumen and content of liquid with conventional MR images and MRCP without need for oral contrast agent.

Fig. 8 Annular pancreas. On axial T2-weighted MR image (A), pancreatic tissue (black arrow) that covers postbulbar duodenum (white arrow) anterolaterally is detected in accordance with incomplete annular pancreas. On magnetic resonance cholangiopancreatography (MRCP) image of another patient (B), aberrant pancreatic duct is superimposed with 2nd portion of duodenum (arrow). Annular pancreas is abnormal pancreatic tissue band that covers 2nd part of duodenum circumferentially. If complete ring is formed, total duodenal obstruction after birth may occur. If ring is incomplete, obstruction may come to clinical attention much later or may be asymptomatic. MRCP is best non-invasive examination method that reveals ductal anatomy, and with MRI, pathologies can be detected such as chronic pancreatitis, pancreas divisum, and polysplenia that are highly encountered in annular pancreas compared with in general population.
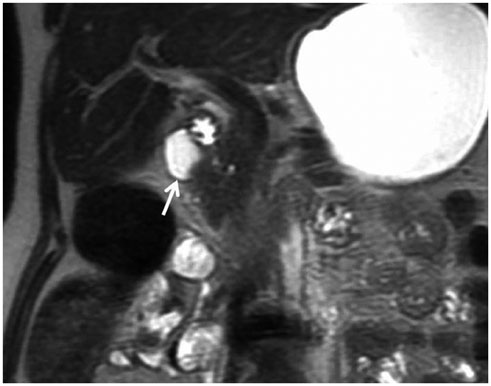
Fig. 9 Duplication cyst. On these coronal T2-weighted MR images, at lateral wall of 2nd portion of duodenum medial to gallbladder, smooth, thin-walled cystic structure (arrow) was noted. Duplication cysts are often encountered incidentally and may cause obstruction and pancreatitis because of their critical location. With MRI, cystic nature and relationship with adjacent structures can be revealed. Duplication cysts need to be differentiated from other cystic lesions (such as choledochal cysts and pancreatic pseudocysts) that may be seen in this location.

Fig. 10 Choledochocele. On coronal T2-weighted (A) and magnetic resonance cholangiopancreatography (B) images, cystic dilatation of distal end of choledochus is noted at level of major papilla (arrow). Cystic dilatation of intraduodenal segment of choledochus is called choledochocele, which is consistent with type-III choledochal cysts according to Todani classification.
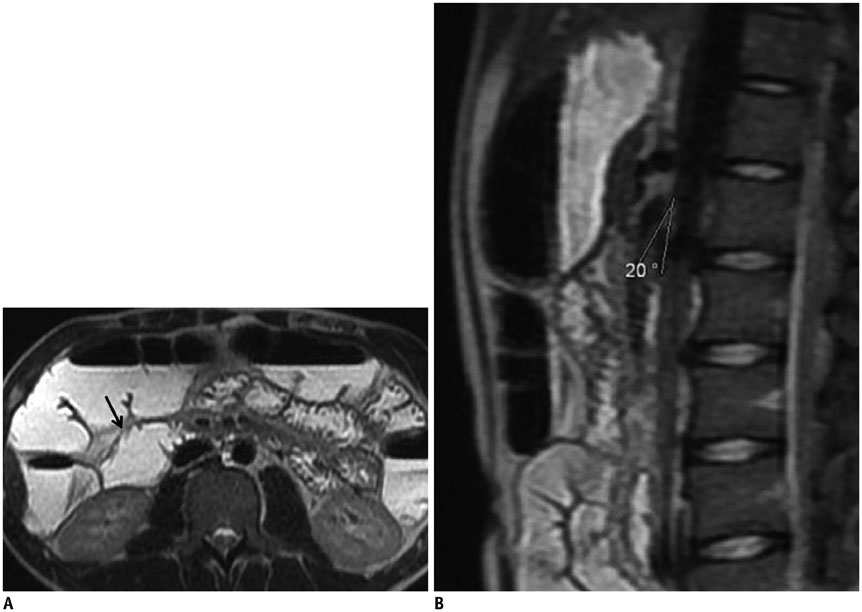
Fig. 11 Dilated duodenum secondary to superior mesenteric artery (SMA) syndrome. On axial (A) T2-weighted MR image, 2nd portion of duodenum is dilated and measures 4 cm (arrow). On sagittal image (B), it is detected that angle between aorta and SMA is narrowed (SMA syndrome). SMA syndrome can be diagnosed in clinically suspected cases on MRI by showing that aortomesenteric angle and distance are less than normal in reconstructed images and by dilatation proximal to obstruction. In barium studies, dilatation in duodenum, barium retention and vertical vascular external impression in 3rd segment are positive signs for SMA syndrome. However, these radiographic symptoms are non-specific, and they may also be seen in diseases such as scleroderma, diabetes, pancreatitis, and peptic ulcer.
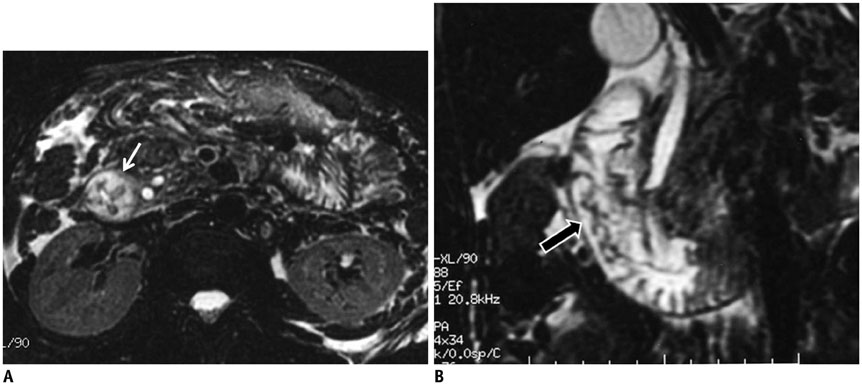
Fig. 12 Duodenal wall thickening secondary to acute pancreatitis. In patient with acute pancreatitis, on axial (A) and coronal (B) fat-suppressed T2-weighted MR images, mural thickening and edema in second portion of duodenum are depicted (white arrow in A, black arrow in B). Pancreatitis is most common inflammatory process that affects duodenum. Inflammation of pancreas and release of exocrine enzymes may lead to mild to severe duodenal edema and gastric outlet obstruction. Moreover, in severe pancreatitis, intramural hematoma may also develop.
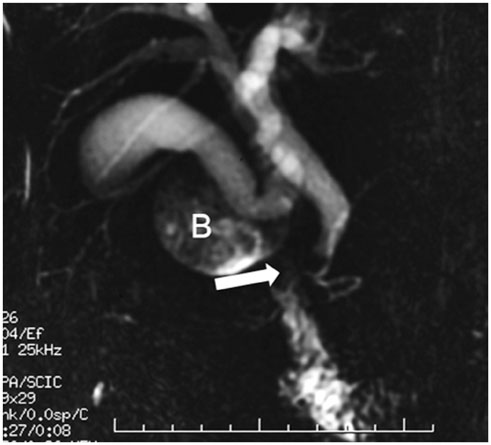
Fig. 13 Postbulbar stenosis. In this patient with gastrojejunostomy, postbulbar ulcer stenosis is shown on magnetic resonance cholangiopancreatography image. In addition, major papilla appears to be retracted cranially to bulbus, producing hook-shaped configuration. Intra- and extrahepatic biliary ducts appear mildly dilated. B = duodenal bulbus
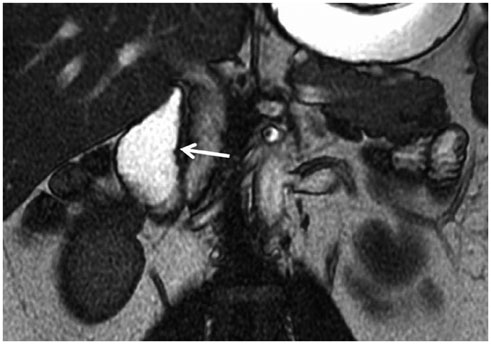
Fig. 14 Duodenal involvement of celiac disease. In this 32-year-old male patient with celiac disease, on coronal fast imaging employing steady-state acquisition MR image, mucosal folds of 2nd portion of duodenum appear indistinct and obscured (arrow). Among duodenal findings of celiac disease, decrease in number of mucosal folds, focal mucosal erosions, mural asymmetry, diffuse and nodular thickening of mucosal folds can be mentioned. Risk of adenocarcinoma and lymphoma increases in celiac patients, and MRI can be used for early diagnosis.
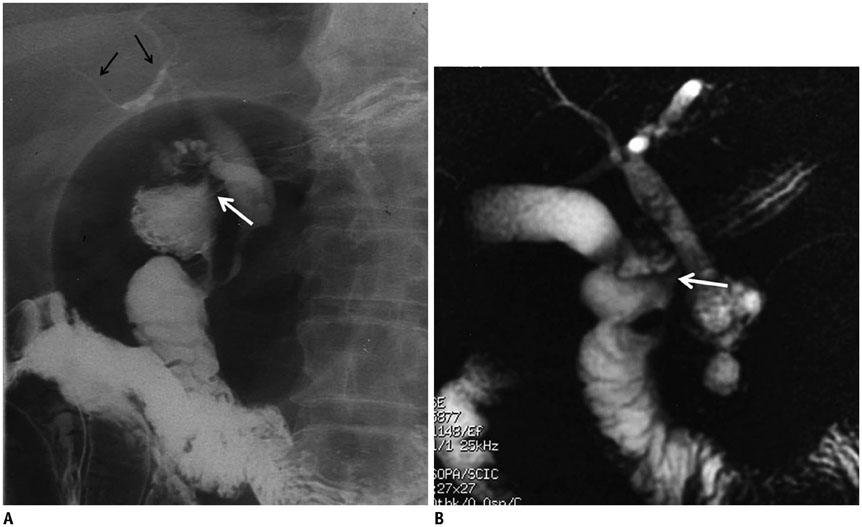
Fig. 15 Choledochoduodenal fistula. In this patient with jaundice, fistula tract between choledochus and duodenum (white arrow) is depicted on barium studies (A) and magnetic resonance cholangiopancreatography (MRCP) image (B). In barium study, filling of bile ducts with contrast medium through fistula is apparent (black arrows in A). Spontaneous bilioenteric fistulas most commonly occur secondary to gallstones and less often from peptic ulcer, malignancy and trauma. Barium studies are more informative and demonstrate fistula itself or reflux of contrast material into biliary system. MRI is valuable for depicting direct communication between biliary system and duodenum by means of MRCP, and it is also superior to other techniques in demonstrating primary pathology or underlying causes.
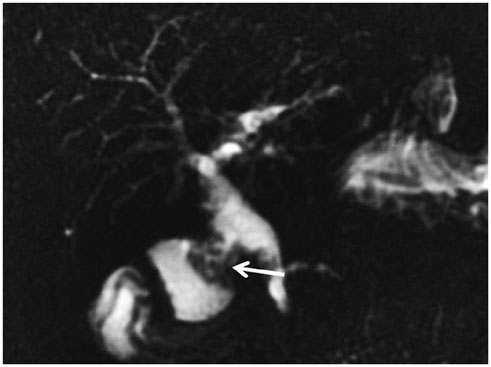
Fig. 16 Choledochoduodenostomy. In this patient with chronic pancreatitis and repetitive cholangitis attacks, anastomosis between choledochus and duodenum (choledochoduodenostomy) is detected on magnetic resonance cholangiopancreatography (arrow). Intrahepatic bile ducts are mildly dilated and irregular because of cholangitis.

Fig. 17 Pseudocyst in duodenum wall. On magnetic resonance cholangiopancreatography (MRCP) (A) and axial T2-weighted MR images (B), cystic lesion consistent with pseudocyst is seen at lateral wall of duodenum in patient with chronic pancreatitis (black arrows in A and B). On MRCP image, pancreatic duct is dilated and irregular because of chronic pancreatitis (arrowhead in A). In pancreatitis, depending on depth of penetration, pseudocysts settle either between serosa and muscular layer or between muscular layer and mucosa. With accumulation of secretion and increase of pressure, obstruction in intestinal lumen and gastric outlet syndrome may occur. Tubular shape of pseudocyst that complies with progress of intestinal wall and abrupt flattening on intestine wall are findings that indicate intramural settlement. Duplication cysts and choledochocele should be considered in differential diagnosis.
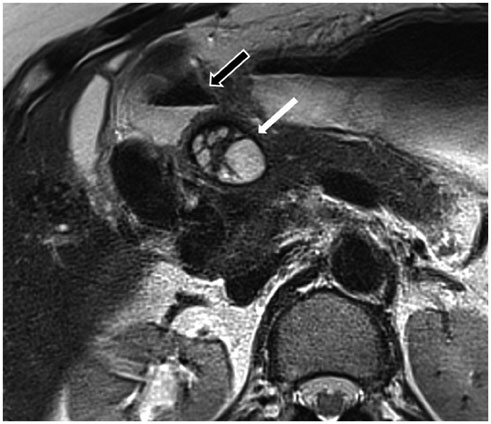
Fig. 18 External compression of duodenum by hydatid cyst. On T2-weighted axial MR image, multiloculated, thick-walled cystic lesion with internal septations is seen at level of pancreatic head-neck junction (white arrow). Lesion slightly compresses duodenum (black arrow) medially from right.
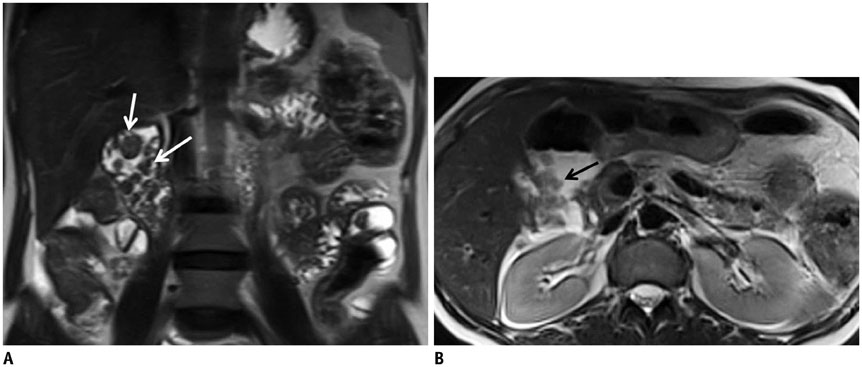
Fig. 19 Peutz-Jeghers syndrome (PJS). In this 41-year-old female patient, multiple polypoid lesions protruding into lumen (arrows) are seen in duodenum on coronal (A) and axial (B) T2-weighted MR images. On more caudal sections, many polyps are also present in jejunum, ileum and colon. PJS is also known as hamartomatous polyposis.

Fig. 20 Ampullary carcinoma. At level of ampulla of Vater, nodular mass that protrudes to lumen (arrow) is seen on fat-suppressed T2-weighted axial images (A). On magnetic resonance cholangiopancreatography (B), distal end of choledochus ends abruptly (white arrow) and bile ducts (arrowheads) and pancreatic duct (black arrow) are dilated because of papillary obstruction. If mass lesion cannot be discriminated on MRI, prominent duodenal papilla may be only sign of ampullary cancer. If marked or abrupt dilation of distal choledochus or pancreatic duct is encountered in patient who has no findings of gallstones or pancreatitis, ampullary carcinoma should be considered in differential diagnosis.

Fig. 21 Adenocarcinoma. Circumferential wall thickening of duodenum is detected on axial fast spin echo T2-weighted image (arrow in A) in 73-year-old patient with epigastric pain. In another patient, diffuse irregular mural thickening (arrow in B) causing luminal stenosis in 3rd and 4th segments of duodenum is demonstrated in MRI small-bowel follow-through image (histopathology: adenocarcinoma). In differential diagnosis of adenocarcinoma, carcinoid tumor, lymphoma, and metastasis should be taken into consideration.
Reference
-
1. Van Hoe L, Gryspeerdt S, Vanbeckevoort D, De Jaegere T, Van Steenbergen W, Dewandel P, et al. Normal Vaterian sphincter complex: evaluation of morphology and contractility with dynamic single-shot MR cholangiopancreatography. AJR Am J Roentgenol. 1998; 170:1497–1500.2. Staritz M. Pharmacology of the sphincter of Oddi. Endoscopy. 1988; 20:Suppl 1. 171–174.3. Horiguchi S, Kamisawa T. Major duodenal papilla and its normal anatomy. Dig Surg. 2010; 27:90–93.4. Kim S, Lee NK, Lee JW, Kim CW, Lee SH, Kim GH, et al. CT evaluation of the bulging papilla with endoscopic correlation. Radiographics. 2007; 27:1023–1038.5. Kim JH, Kim MJ, Chung JJ, Lee WJ, Yoo HS, Lee JT. Differential diagnosis of periampullary carcinomas at MR imaging. Radiographics. 2002; 22:1335–1352.6. Cronin CG, Lohan DG, DeLappe E, Roche C, Murphy JM. Duodenal abnormalities at MR small-bowel follow-through. AJR Am J Roentgenol. 2008; 191:1082–1092.7. Jayaraman MV, Mayo-Smith WW, Movson JS, Dupuy DE, Wallach MT. CT of the duodenum: an overlooked segment gets its due. Radiographics. 2001; 21:S147–S160.8. Zissin R, Osadchy A, Gayer G, Shapiro-Feinberg M. Pictorial review. CT of duodenal pathology. Br J Radiol. 2002; 75:78–84.9. Mazziotti S, Costa C, Ascenti G, Gaeta M, Pandolfo A, Blandino A. MR cholangiopancreatography diagnosis of juxtapapillary duodenal diverticulum simulating a cystic lesion of the pancreas: usefulness of an oral negative contrast agent. AJR Am J Roentgenol. 2005; 185:432–435.10. Hwang JI, Chiang JH, Yu C, Cheng HC, Chang CY, Mueller PR. Pictorial review: Radiological diagnosis of duodenal abnormalities. Clin Radiol. 1998; 53:323–332.11. Tsitouridis I, Emmanouilidou M, Goutsaridou F, Kokozidis G, Kalambakas A, Papastergiou C, et al. MR cholangiography in the evaluation of patients with duodenal periampullary diverticulum. Eur J Radiol. 2003; 47:154–160.12. Takamatsu S, Gabata T, Matsui O, Noto M, Ninomiya I, Nonomura A. Intraluminal duodenal diverticulum: MR findings. Abdom Imaging. 2006; 31:39–42.13. Tu AS, Tran MH, Larsen CR. CT-appearance of intraluminal duodenal diverticulum. The "halo" sign. Comput Med Imaging Graph. 1998; 22:81–83.14. Afridi SA, Fichtenbaum CJ, Taubin H. Review of duodenal diverticula. Am J Gastroenterol. 1991; 86:935–938.15. Tasu JP, Rocher L, Amouyal P, Lorand I, Rondeau Y, Buffet C, et al. Intraluminal duodenal diverticulum: radiological and endoscopic ultrasonography findings of an unusual cause of acute pancreatitis. Eur Radiol. 1999; 9:1898–1900.16. Finnie IA, Ghosh P, Garvey C, Poston GJ, Rhodes JM. Intraluminal duodenal diverticulum causing recurrent pancreatitis: treatment by endoscopic incision. Gut. 1994; 35:557–559.17. Berrocal T, Torres I, Gutiérrez J, Prieto C, del Hoyo ML, Lamas M. Congenital anomalies of the upper gastrointestinal tract. Radiographics. 1999; 19:855–872.18. Lee NK, Kim S, Jeon TY, Kim HS, Kim DH, Seo HI, et al. Complications of congenital and developmental abnormalities of the gastrointestinal tract in adolescents and adults: evaluation with multimodality imaging. Radiographics. 2010; 30:1489–1507.19. Sandrasegaran K, Patel A, Fogel EL, Zyromski NJ, Pitt HA. Annular pancreas in adults. AJR Am J Roentgenol. 2009; 193:455–460.20. Türkvatan A, Erden A, Türkoğlu MA, Yener Ö. Congenital variants and anomalies of the pancreas and pancreatic duct: imaging by magnetic resonance cholangiopancreaticography and multidetector computed tomography. Korean J Radiol. 2013; 14:905–913.21. Macpherson RI. Gastrointestinal tract duplications: clinical, pathologic, etiologic, and radiologic considerations. Radiographics. 1993; 13:1063–1080.22. Rice CA, Anderson TM, Sepahdari S. Computed tomography and ultrasonography of carcinoma in duplication cysts. J Comput Assist Tomogr. 1986; 10:233–235.23. Can MF, Kaymakc¸ioğlu N, Yağci G, Görgülü S, Tufan T. An adult choledochocele case presented with gastric outlet obstruction: a rare presentation. Turk J Gastroenterol. 2006; 17:70–73.24. Jabłońska B. Biliary cysts: etiology, diagnosis and management. World J Gastroenterol. 2012; 18:4801–4810.25. Lee HK, Park SJ, Yi BH, Lee AL, Moon JH, Chang YW. Imaging features of adult choledochal cysts: a pictorial review. Korean J Radiol. 2009; 10:71–80.26. Konen E, Amitai M, Apter S, Garniek A, Gayer G, Nass S, et al. CT angiography of superior mesenteric artery syndrome. AJR Am J Roentgenol. 1998; 171:1279–1281.27. Gustafsson L, Falk A, Lukes PJ, Gamklou R. Diagnosis and treatment of superior mesenteric artery syndrome. Br J Surg. 1984; 71:499–501.28. Kennedy KV, Yela R, Achalandabaso Mdel M, Martín-Pérez E. Superior mesenteric artery syndrome: diagnostic and therapeutic considerations. Rev Esp Enferm Dig. 2013; 105:236–238.29. Felton BM, White JM, Racine MA. An uncommon case of abdominal pain: superior mesenteric artery syndrome. West J Emerg Med. 2012; 13:501–502.30. Bauer S, Karplus R, Belsky V, Mha HA. Superior mesenteric artery syndrome: a forgotten entity. Isr Med Assoc J. 2013; 15:189–191.31. Al-Rashedy M, El-Dhuwaib Y, Issa M, Ballester P, Ammori BJ. Laparoscopic management of acquired benign duodenal strictures in adults. Internet J Surg. 2005; 6:14.32. Lee HJ, Ha HK, Kim MH, Jeong YK, Kim PN, Lee MG, et al. ERCP and CT findings of ectopic drainage of the common bile duct into the duodenal bulb. AJR Am J Roentgenol. 1997; 169:517–520.33. Dadzan E, Akhondi H. Choledochoduodenal fistula presenting with pneumobilia in a patient with gallbladder cancer: a case report. J Med Case Rep. 2012; 6:61.34. Okabe T, Ohwada S, Ogawa T, Takeyoshi I, Sato Y, Kamoshita N, et al. Gallbladder carcinoma with choledochoduodenal fistula: a case report with surgical treatment. Hepatogastroenterology. 1999; 46:1660–1663.35. Aramaki M, Ikeda M, Kawanaka H, Nishijima N, Tsutsumi N, Kano T, et al. Choledochoduodenostomy: simple side-to-side anastomosis. J Hepatobiliary Pancreat Surg. 2000; 7:486–488.36. McCowin MJ, Federle MP. Computed tomography of pancreatic pseudocysts of the duodenum. AJR Am J Roentgenol. 1985; 145:1003–1007.37. Bellon EM, George CR, Schreiber H, Marshall JB. Pancreatic pseudocysts of the duodenum. AJR Am J Roentgenol. 1979; 133:827–831.38. Yano T, Yamamoto H. Vascular, polypoid, and other lesions of the small bowel. Best Pract Res Clin Gastroenterol. 2009; 23:61–74.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Annular Pancreas with a Duodenal Web: a Rare Presentation with Simultaneous Intrinsic and Extrinsic Duodenal Obstruction
- A Preliminary Study for the Development and the Standardization of Korean Version of the Intrinsic/Extrinsic Religious Orientation Scale
- Production of interleukin 4 and interferon gamma in CD8+ T cells from patients with intrinsic and extrinsic asthma
- Age-related Changes in the Frequency of Intrinsic and Extrinsic Atopic Dermatitis: A Single-center Retrospective Study
- Vascular Anatomy of Spinal Cord
