J Korean Med Assoc.
2012 Jan;55(1):31-36.
Treatment of fecal incontinence
- Affiliations
-
- 1Department of Gastroenterology, Ajou University School of Medicine, Suwon, Korea. kjleemd@hotmail.com
Abstract
- Fecal incontinence is defined as either the involuntary passage of gas or stool or the inability to control the passage of fecal contents through the anus. Patients are reluctant to report fecal incontinence, resulting in underestimated prevalence. Studies have reported that its prevalence ranges from 2% to 20%. Diverse causes are involved in the generation of fecal incontinence. Fecal incontinence leads to a loss of self-esteem, social isolation, and a diminished quality of life. Antidiarrheals are useful for diarrhea with incontinence. Biofeedback therapy and exercise therapies may be helpful, particularly in patients with weak sphincters and/or impaired rectal sensation. Sacral nerve stimulation can be an option if other treatments have not been successful. Although some studies have shown the efficacy of injectable bulking agents, data on their long-term outcome and experience are lacking. Sphincteroplasty can be considered in selected patients who have failed nonsurgical measures or biofeedback therapy. A colostomy is a less preferable option. The various treatment options can be chosen with an individualized approach, depending on the causes of fecal incontinence, the action mechanism of treatment, comorbidities, general condition, and procedure-related risks.
MeSH Terms
Figure
-
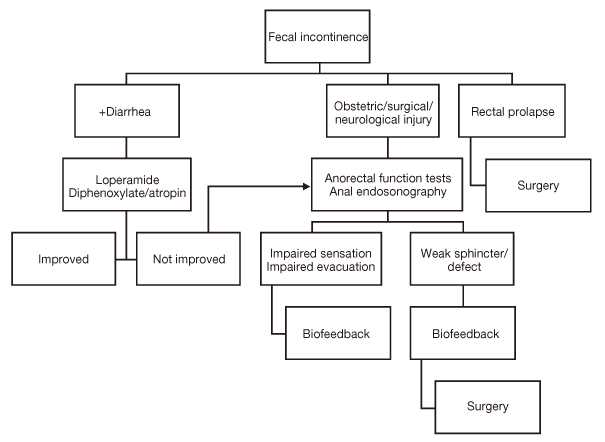
Figure 1 Algorithmic approach for the management of patients with fecal incontinence.
Reference
-
1. Madoff RD, Parker SC, Varma MG, Lowry AC. Faecal incontinence in adults. Lancet. 2004. 364:621–632.
Article2. Nelson RL. Epidemiology of fecal incontinence. Gastroenterology. 2004. 126:1 Suppl 1. S3–S7.
Article3. Ho YH, Muller R, Veitch C, Rane A, Durrheim D. Faecal incontinence: an unrecognised epidemic in rural North Queensland? Results of a hospital-based outpatient study. Aust J Rural Health. 2005. 13:28–34.
Article4. Rao SS. American College of Gastroenterology Practice Parameters Committee. Diagnosis and management of fecal incontinence. American College of Gastroenterology Practice Parameters Committee. Am J Gastroenterol. 2004. 99:1585–1604.5. Law PJ, Kamm MA, Bartram CI. Anal endosonography in the investigation of faecal incontinence. Br J Surg. 1991. 78:312–314.
Article6. Woodfield CA, Krishnamoorthy S, Hampton BS, Brody JM. Imaging pelvic floor disorders: trend toward comprehensive MRI. AJR Am J Roentgenol. 2010. 194:1640–1649.
Article7. Wald A. Fecal incontinence. Curr Treat Options Gastroenterol. 2005. 8:319–324.
Article8. Santoro GA, Eitan BZ, Pryde A, Bartolo DC. Open study of low-dose amitriptyline in the treatment of patients with idiopathic fecal incontinence. Dis Colon Rectum. 2000. 43:1676–1681.
Article9. Leroi AM, Dorival MP, Lecouturier MF, Saiter C, Welter ML, Touchais JY, Denis P. Pudendal neuropathy and severity of incontinence but not presence of an anal sphincter defect may determine the response to biofeedback therapy in fecal incontinence. Dis Colon Rectum. 1999. 42:762–769.
Article10. Van Tets WF, Kuijpers JH, Bleijenberg G. Biofeedback treatment is ineffective in neurogenic fecal incontinence. Dis Colon Rectum. 1996. 39:992–994.
Article11. Norton C, Cody JD, Hosker G. Biofeedback and/or sphincter exercises for the treatment of faecal incontinence in adults. Cochrane Database Syst Rev. 2006. 3:CD002111.
Article12. Leroi AM, Parc Y, Lehur PA, Mion F, Barth X, Rullier E, Bresler L, Portier G, Michot F. Study Group. Efficacy of sacral nerve stimulation for fecal incontinence: results of a multicenter double-blind crossover study. Ann Surg. 2005. 242:662–669.13. Mellgren A, Wexner SD, Coller JA, Devroede G, Lerew DR, Madoff RD, Hull T. SNS Study Group. Long-term efficacy and safety of sacral nerve stimulation for fecal incontinence. Dis Colon Rectum. 2011. 54:1065–1075.
Article14. Brouwer R, Duthie G. Sacral nerve neuromodulation is effective treatment for fecal incontinence in the presence of a sphincter defect, pudendal neuropathy, or previous sphincter repair. Dis Colon Rectum. 2010. 53:273–278.
Article15. Vaizey CJ, Kamm MA, Nicholls RJ. Recent advances in the surgical treatment of faecal incontinence. Br J Surg. 1998. 85:596–603.
Article16. Tan JJ, Chan M, Tjandra JJ. Evolving therapy for fecal incontinence. Dis Colon Rectum. 2007. 50:1950–1967.
Article
