Transscleral Fixation of Intraocular Lenses Using Modified Injector
- Affiliations
-
- 1Department of Ophthalmology, Hanyang University Guri Hospital, Hanyang University College of Medicine, Guri, Korea. ocularimmunity@gmail.com
- KMID: 2339039
- DOI: http://doi.org/10.3341/jkos.2015.56.3.345
Abstract
- PURPOSE
To evaluate the clinical stability and outcomes of 3-piece intraocular lens (IOL) transscleral fixation surgery using a modified injector.
METHODS
We have modified and used the Sapphire unfolder injector system (Allergan(R), USA). This involved, cutting a slit longitudinally at the terminal part of the injector so that a thread could pass through it freely. After a conjunctival peritomy created at 2 and 8 o'clock, a long curved needle with double-armed 10-0 polypropylene is passed through the exposed sclera. Two pieces of suture are withdrawn through the 2.8 mm corneal incision and 1 suture (from 8 o'clock) is passed through the opening of the cartridge and then tied to the leading haptic. Next, the IOL was implanted with the cartridge and then inserted through the corneal incision site. The other suture (from 2 o'clock) is tied to the haptic on the opposite side and inserted.
RESULTS
The study included 20 eyes of 20 patients with a mean age of 62.8 years at the initial visit. There were no complications, such as vitreous hemorrhage, retinal detachment, glaucoma, corneal edema, or iris injury. While the knot fixed to the leading haptic of IOL passed by the cartridge, there was no change of position. During the follow-up period, IOL dislocation did not occur and the corrected visual acuity and corneal astigmatism improved significantly.
CONCLUSIONS
This technique is an effective procedure for minimizing entangled thread and corneal astigmatism.
Keyword
MeSH Terms
Figure
-

Figure 1. Modification of injector system: (Upper)-Injector before modification. (Lower)-After modification. Grinding between tip of injector and cartridge equip space was done.

Figure 2. The method of transscleral fixation using modified injector system. (A) The 10-0 polypropylene from the 7-o’clock posi-tion of the sclera is passed through the cartridge. (B) The thread is fixed to the leading haptic 2 mm away from the terminal end. (C) The cartridge is mounted on the injector. 10-0 polypropylene tied to the haptic is passed through the modified side groove of the injector. (D) Combined injector. 10-0 polypropylene is shown at the end of the injector.
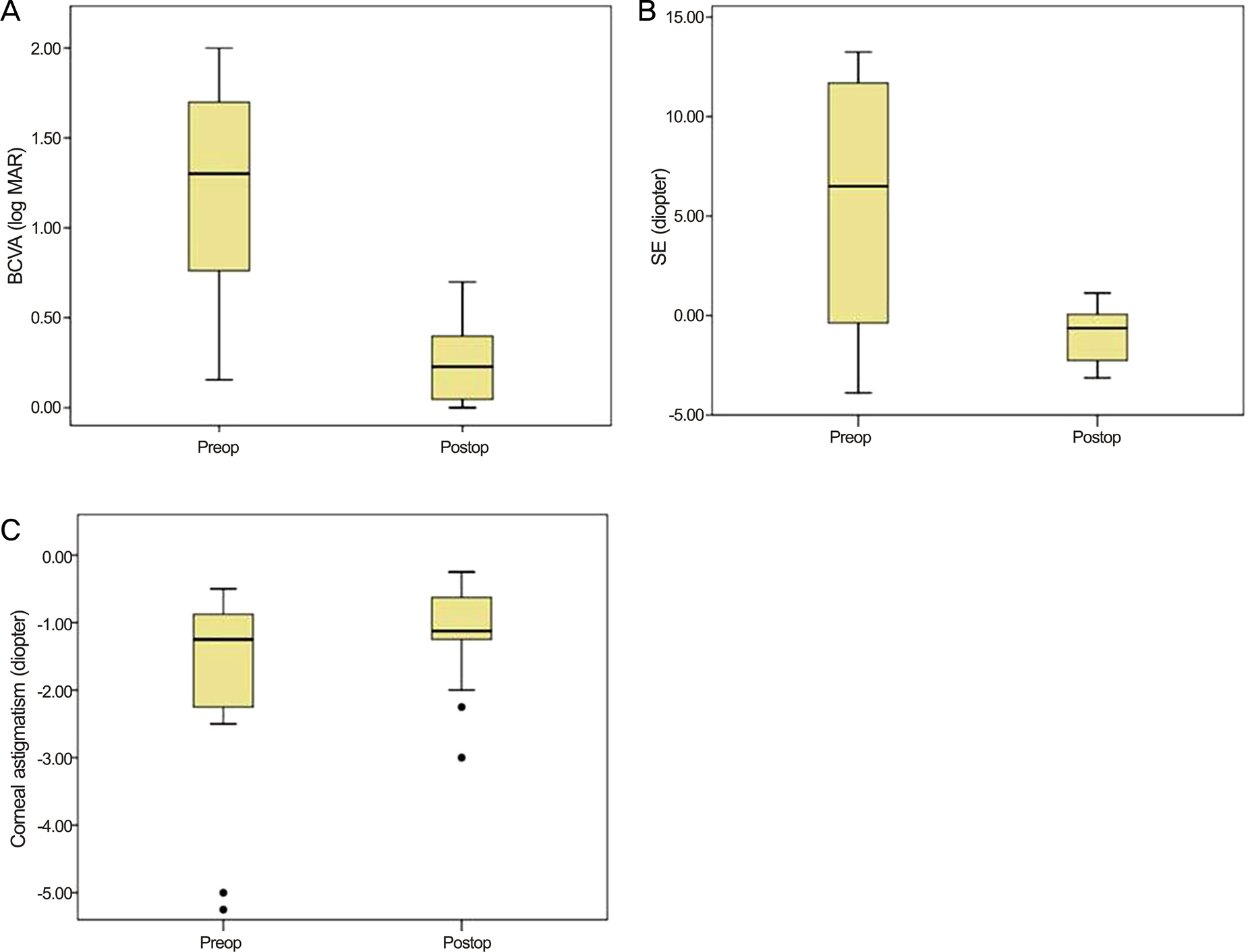
Figure 3. Clinical outcomes of transscleral fixation using injector system. (A) Mean best corrected visual acuity (BCVA, log MAR), (B) SE (diopter) and (C) corneal astigmatism (diopter) of preoperative and posterative data. All clinical outcomes showed statistically significant differences after surgery ( p < 0.001, p = 0.004, p = 0.012). SE = spherical equivalent.
Reference
-
References
1. Duffey RJ, Holland EJ, Agapitos PJ, Lindstrom RL. Anatomic study of transsclerally sutured intraocular lens implantation. Am J Ophthalmol. 1989; 108:300–9.
Article2. Chan CK. An improved technique for management of dislocated posterior chamber implants. Ophthalmology. 1992; 99:51–7.
Article3. Hayashi K, Hayashi H, Nakao F, Hayashi F. Intraocular lens tilt and decentration, anterior chamber depth, and refractive error after transscleral suture fixation surgery. Ophthalmology. 1999; 106:878–82.4. Szurman P, Petermeier K, Jaissle GB, Bartz-Schmidt KU. A new small-incision technique for injector implantation of transsclerally sutured foldable lenses. Ophthalmic Surg Lasers Imaging. 2007; 38:76–80.
Article5. Sundmacher R, Althaus C, Wester R. Experience with transscleral fixation of posterior chamber lenses. Graefes Arch Clin Exp Ophthalmol. 1991; 229:512–6.
Article6. Solomon K, Gussler JR, Gussler C, Van Meter WS. Incidence and management of complications of transsclerally sutured posterior chamber lenses. J Cataract Refract Surg. 1993; 19:488–93.
Article7. Moon AR, Moon NJ, Choi KY. Long-term results and complications using scleral-fixated posterior chamber intraocular lenses. J Korean Ophthalmol Soc. 1996; 37:1283–92.8. Kaynak S, Ozbek Z, Pasa E, et al. Transscleral fixation of foldable intraocular lenses. J Cataract Refract Surg. 2004; 30:854–7.
Article9. Gills JP, Sanders DR. Use of small incisions to control induced astigmatism and inflammation following cataract surgery. J Cataract Refract Surg. 1991; 17(Suppl):740–4.
Article10. Nielsen PJ. Prospective evaluation of surgically induced astigmatism and astigmatic keratotomy effects of various self-sealing small incisions. J Cataract Refract Surg. 1995; 21:43–8.
Article11. Lever J, Dahan E. Opposite clear corneal incisions to correct pre- existing astigmatism in cataract surgery. J Cataract Refract Surg. 2000; 26:803–5.12. Choi KS, Park SY, Sun HJ. Transscleral fixation by injector implantation of a foldable intraocular lens. Ophthalmic Surg Lasers Imaging. 2010; 41:272–5.
Article13. Roger FS. Cataract Surgery-Techniques, Complications and Management. 2nd ed.Saunders;2004. p. 409–10.14. Kim DH, Heo JW, Hwang SW, et al. Modified transscleral fixation using combined temporary haptic externalization and injector intraocular lens implantation. J Cataract Refract Surg. 2010; 36:707–11.
Article15. Roh KH, Park MJ, Choi KS, Lee SJ. Scleral fixation of foldable intraocular lenses using injector. J Korean Ophthalmol Soc. 2007; 48:167–71.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Effect of Distances Between Corneoscleral Limbus and Transscleral Sutures on Vision and Refraction in Eyes with Posterior Chamber Intraocular Lens Implanted by Transscleral Suture Fixation
- Comparison of Clinical Results between Sulcus Insertion and Transscleral Fixation of Intraocular Lenses
- Knotless External Fixation Technique for Posterior Chamber Intraocular Lens Transscleral Fixation: A 5-Case Analysis
- The Role of Vitrectomy in Transscleral Fixation of Posterior Chamber Intraocular Lens
- Implantation of Posterior Chamber Intraocular Lens by Transscleral Suture Fixation: Long-term Results
