The Evaluation of Prognostic Factors after Vitrectomy for Lamellar Macular Hole Using Optical Coherence Tomography
- Affiliations
-
- 1Sungmo Eye Hospital, Busan, Korea. heesyoon@dreamwiz.com
- KMID: 2338976
- DOI: http://doi.org/10.3341/jkos.2014.55.12.1853
Abstract
- PURPOSE
To evaluate the prognostic factors that predict visual outcome after vitrectomy for lamellar macular hole using optical coherence tomography (OCT).
METHODS
This study included 26 eyes that underwent pars plana vitrectomy, epiretinal membrane removal, and internal limiting membrane peeling for lamellar macular hole. The maximum parafoveal thickness, maximum height and diameter of lamellar macular hole, maximum height and diameter of intraretinal splitting, thinnest foveal floor thickness, and inner segment/outer segment disruption length on preoperative OCT image were investigated for prognostic factors that predict visual outcome.
RESULTS
The mean follow-up period was 32.2 months and the mean best corrected visual acuity improved significantly after vitrectomy from log MAR 0.47 +/- 0.32 to log MAR 0.23 +/- 0.23. The postoperative visual acuity correlated significantly with preoperative visual acuity, thinnest foveal floor thickness and inner segment/outer segment disruption length, but not with maximum parafoveal thickness, maximum height and diameter of lamellar macular hole and maximum height and diameter of intraretinal splitting.
CONCLUSIONS
The thinnest foveal floor thickness and inner segment/outer segment disruption length on preoperative OCT image were significant prognostic factors.
MeSH Terms
Figure
-
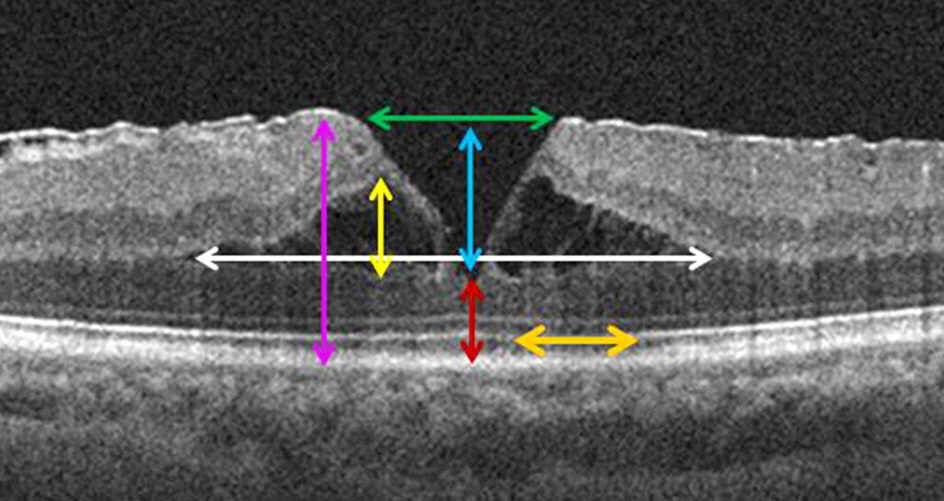
Figure 1. Presumed prognostic factor of spectral-domain optical coherence tomography. The pink arrow indicates the maximum parafovea thickness; the blue arrow indicates the maximum height of lamellar macular hole; the green arrow indicates the maximum diameter of lamellar macular hole; the yellow arrow indicates the maximum height of intraretinal splitting; the white arrow indicates the maximum diameter of intraretinal splitting; the red arrow indicates thinnest foveal floor thickness; the orange arrow indicates inner segment/outer segment disruption length.
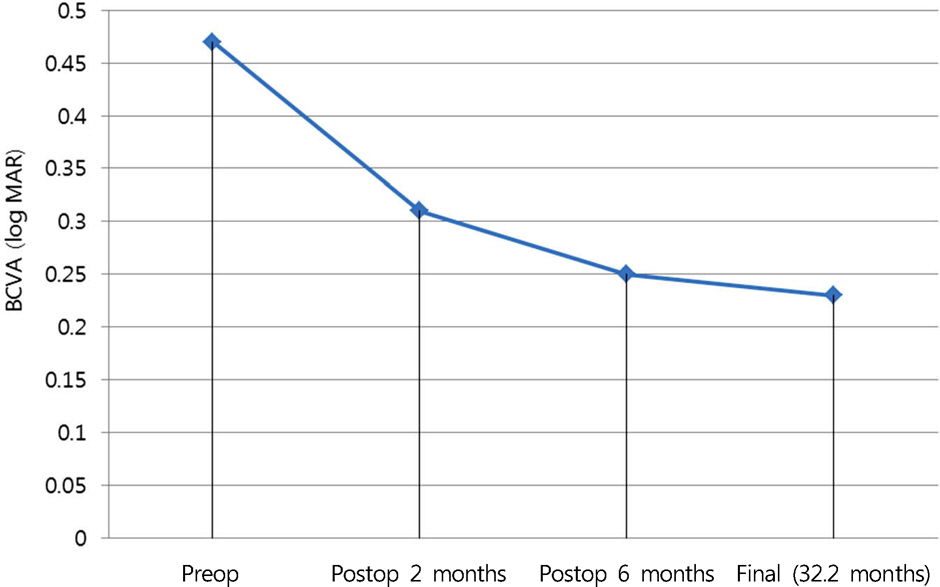
Figure 2. Mean best corrected visual acuity (log MAR) changes after treatment. BCVA of 26 eyes showed statistically significant improvement at each time after treatment (p < 0.05, Wilcoxon signed rank test). BCVA = best corrected visual acuity.
Reference
-
References
1. Gass JD. Lamellar macular hole: a complication of cystoid macular edema after cataract extraction: a clinicopathologic case report. Trans Am Ophthalmol Soc. 1975; 73:231–50.2. Witkin AJ, Ko TH, Fujimoto JG, et al. Redefining lamellar holes and the vitreomacular interface: an ultrahigh-resolution optical coherence tomography study. Ophthalmology. 2006; 113:388–97.
Article3. Theodossiadis PG, Grigoropoulos VG, Emfietzoglou I, et al. Evolution of lamellar macular hole studied by optical coherence tomography. Graefes Arch Clin Exp Ophthalmol. 2009; 247:13–20.
Article4. Chen JC, Lee LR. Clinical spectrum of lamellar macular defects including pseudoholes and pseudocysts defined by optical coherence tomography. Br J Ophthalmol. 2008; 92:1342–6.
Article5. Takahashi H, Kishi S. Tomographic features of a lamellar macular hole formation and a lamellar hole that progressed to a full-thickness macular hole. Am J Ophthalmol. 2000; 130:677–9.
Article6. Lee SJ, Jang SY, Moon D, et al. Long-term surgical outcomes after vitrectomy for symptomatic lamellar macular holes. Retina. 2012; 32:1743–8.
Article7. Michalewska Z, Michalewski J, Odrobina D, et al. Surgical treatment of lamellar macular holes. Graefes Arch Clin Exp Ophthalmol. 2010; 248:1395–400.
Article8. Haouchine B, Massin P, Gaudric A. Foveal pseudocyst as the first step in macular hole formation: a prospective study by optical coherence tomography. Ophthalmology. 2001; 108:15–22.9. Garretson BR, Pollack JS, Ruby AJ, et al. Vitrectomy for a symptomatic lamellar macular hole. Ophthalmology. 2008; 115:884–6.e1.
Article10. Choi WS, Kim SW, Lee WS, et al. Visual and surgical outcomes of lamellar macular hole. J Korean Ophthalmol Soc. 2012; 53:1291–5.
Article11. Suh MH, Seo JM, Park KH, Yu HG. Associations between macular findings by optical coherence tomography and visual outcomes after epiretinal membrane removal. Am J Ophthalmol. 2009; 147:473–80.e3.
Article12. Inoue M, Morita S, Watanabe Y, et al. Preoperative inner segment/outer segment junction in spectral-domain optical coherence tomography as a prognostic factor in epiretinal membrane surgery. Retina. 2011; 31:1366–72.
Article13. Lee CS, Koh HJ, Lim HT, et al. Prognostic factors in vitrectomy for lamellar macular hole assessed by spectral-domain optical coherence tomography. Acta Ophthalmol. 2012; 90:e597–602.
Article14. Frangieh GT, Green WR, Engel HM. A histopathologic study of macular cysts and holes. Retina. 1981; 1:311–36.
Article15. Guyer DR, Green WR, de Bustros S, Fine SL. Histopathologic features of idiopathic macular holes and cysts. Ophthalmology. 1990; 97:1045–51.
Article16. Chang LK, Koizumi H, Spaide RF. Disruption of the photoreceptor inner segment-outer segment junction in eyes with macular holes. Retina. 2008; 28:969–75.
Article17. Chung H, Shin CJ, Kim JG, et al. Correlation of microperimetry with fundus autofluorescence and spectral-domain optical coherence tomography in repaired macular holes. Am J Ophthalmol. 2011; 151:128–36.e3.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Evaluation of Prognostic Factors after Vitrectomy for Idiopathic Macular Hole with OCT
- Visual and Surgical Outcomes of Lamellar Macular Hole
- Effects of Vitrectomy on the Treatment of a Lamellar Macular Hole in Highly Myopic Patients
- The Effect of Gas Tamponade with Vitrectomy in Lamellar Macular Hole
- Optical Coherence Tomographic Evaluation of Impending Idiopathic Macular Hole Repaired by Vitrectomy
