J Korean Ophthalmol Soc.
2014 Dec;55(12):1772-1778. 10.3341/jkos.2014.55.12.1772.
Current Status and Future Expectations of Cataract Surgery in Korea: KNHANES IV
- Affiliations
-
- 1Institute of Vision Research, Department of Ophthalmology, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea. SEMEKIM@yuhs.ac
- 2The Epidemiologic Survey Committee in the Korean Ophthalmological Society, Seoul, Korea.
- KMID: 2338959
- DOI: http://doi.org/10.3341/jkos.2014.55.12.1772
Abstract
- PURPOSE
To identify socio-demographic factors in cataract surgery in Korea and expect future effect of the bundle of service system.
METHODS
We analyzed the number of people undergoing cataract surgery and associated factors such as surgery ratio, region, age, income, and insurance status of 28,980 patients older than 40 years using data from the fifth Korea National Health and Nutrition Examination Survey 2008-2012 (KNHANES).
RESULTS
Among total population in 2012, 47.5% of elderly aged 80 years and older have received cataract surgery. According to region in patients older than 40, Jeollanam-do showed the highest proportion of patients undergoing cataract surgery, at 12%, Daejeon showed the lowest proportion of 3.6%, and Seoul showed 6.8%. Regional analysis was also performed by analyzing the number of cataract patients per ophthalmologist. Jeollanam-do showed the highest with 40,115 patients per ophthalmologist, and Seoul showed the least with 1,094 patients per ophthalmologist. The sociodemographic factors such as education or income, were not associated with cataract surgery after adjusting for age and regional difference. On the other hand, subjects with medicaid were associated with 1.6-fold (95% confidence interval, 1.3-2.0) higher rate of cataract surgery than subjects with national health insurance.
CONCLUSIONS
Regional disparity was found in the cataract surgery rate and surgery rate per an ophthalmologists, whereas sociodemographic factors were not significant in receiving benefits of cataract surgery. Before the amount of bundled payment is changing, down-leveling of quality of care and deepening of disparities among health care provider should be considered.
MeSH Terms
Figure
-
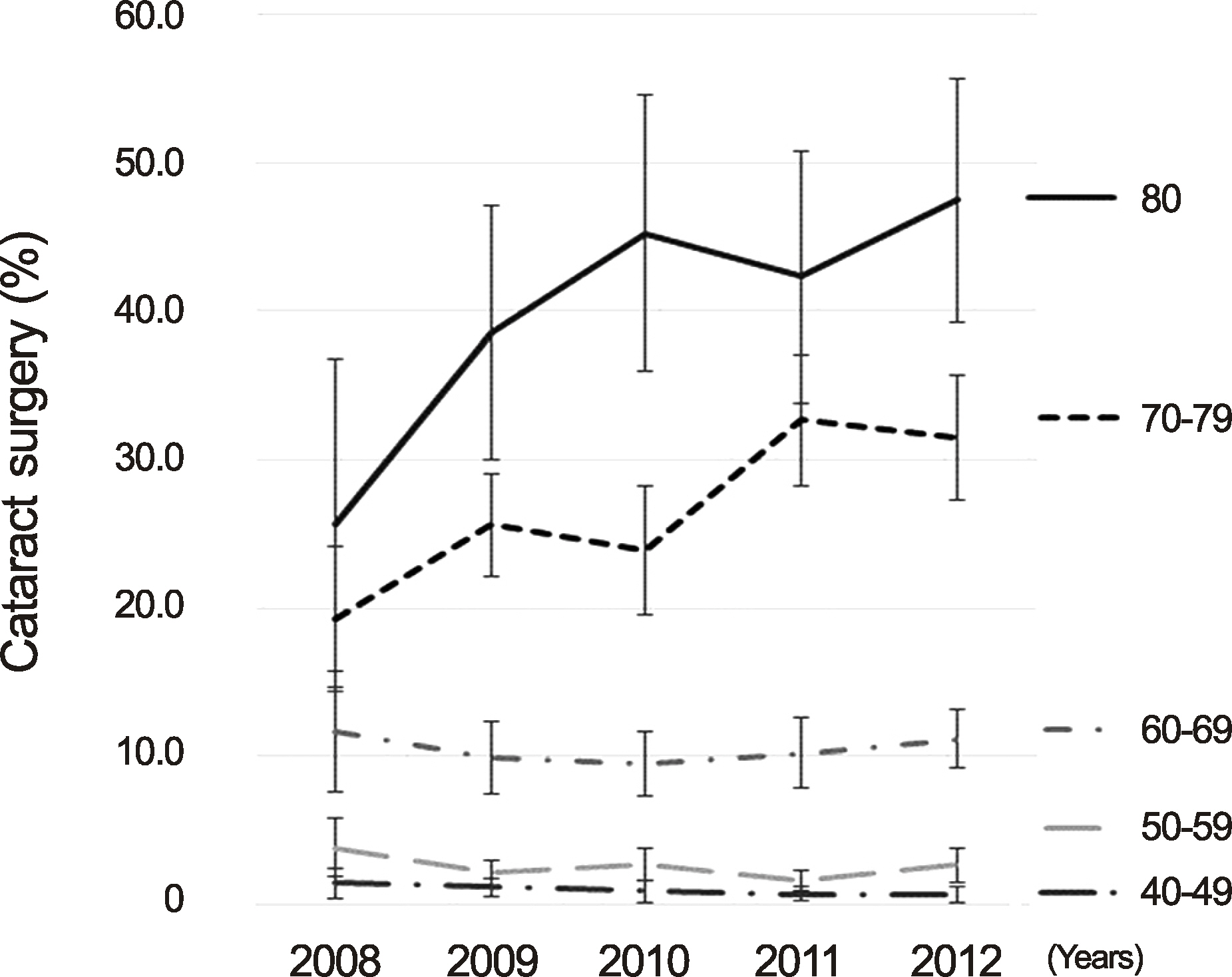
Figure 1. Cataract surgery ratio according to age group and year. Among total population in 2012, 47.5% of elderly aged 80 years and older have received cataract surgery.
Reference
-
References
1. World Health Organization. ICD 10: International statistical classification Of diseases and related health problems. 10th ed.1:1992. p. 429–58.2. Resnikoff S, Pascolini D, Etya'ale D, et al. Global data on visual impairment in the year 2002. Bull World Health Organ. 2004; 82:844–51.3. Thylefors B, Négrel AD, Pararajasegaram R, Dadzie KY. Global data on blindness. Bull World Health Organ. 1995; 73:115–21.4. Rim TH, Kim MH, Kim WC, et al. Cataract subtype risk factors identified from the Korea National Health and Nutrition Examination survey 2008-2010. BMC Ophthalmol. 2014; 14:4.
Article5. Lansingh VC, Carter MJ, Martens M. Global cost-effectiveness of cataract surgery. Ophthalmology. 2007; 114:1670–8.
Article6. Baltussen R, Sylla M, Mariotti SP. Cost-effectiveness analysis of cataract surgery: a global and regional analysis. Bull World Health Organ. 2004; 82:338–45.7. Finger RP, Kupitz DG, Fenwick E, et al. The impact of successful cataract surgery on quality of life, household income and social status in South India. PLoS One. 2012; 7:e44268.
Article8. Zhou JB, Guan HJ, Qu J, et al. A study on the awareness of cataract disease and treatment options in patients who need surgery in a rural area of Eastern China. Eur J Ophthalmol. 2008; 18:544–50.
Article9. Kovai V, Prasadarao BV, Paudel P, et al. Reasons for refusing cataract surgery in illiterate individuals in a tribal area of Andhra Pradesh, India. Ophthalmic Epidemiol. 2014; 21:144–52.
Article10. Rim TH, Park SY, Kim TI. Epidemiological survey regarding cataract awareness in Korea: KNHANES IV. J Korean Ophthalmol Soc. 2013; 54:72–7.
Article11. Mitchell P, Cumming RG, Attebo K, Panchapakesan J. Prevalence of cataract in Australia: the Blue Mountains eye study. Ophthalmology. 1997; 104:581–8.12. Kahn HA, Leibowitz HM, Ganley JP, et al. The Framingham Eye Study. II. Association of ophthalmic pathology with single variables previously measured in the Framingham Heart Study. Am J Epidemiol. 1977; 106:33–41.13. Chung HW, Shyn KH. An epidemiological study for relationship between risk factors and types of cataract. J Korean Ophthalmol Soc. 1995; 36:227–33.14. Williams A, Sloan FA, Lee PP. Longitudinal rates of cataract surgery. Arch Ophthalmol. 2006; 124:1308–14.
Article15. Erie JC, Baratz KH, Hodge DO, et al. Incidence of cataract surgery from 1980 through 2004: 25-year population-based study. J Cataract Refract Surg. 2007; 33:1273–7.
Article16. Gollogly HE, Hodge DO, St Sauver JL, Erie JC. Increasing incidence of cataract surgery: population-based study. J Cataract Refract Surg. 2013; 39:1383–9.
Article17. Rim TH, Byun IH, Kim HS, et al. Factors associated with diabetic retinopathy and nephropathy screening in Korea: the third and fourth Korea National Health and Nutrition Examination Survey (KNHANES III and IV). J Korean Med Sci. 2013; 28:814–20.
Article18. Park EC, Yoo KB, Kim JH, et al. A study on the current state and direction of bundled payment. Research institute for healthcare policy korean medical association institute. 2014.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Epidemiological Survey Regarding Cataract Awareness in Korea: KNHANES IV
- 2006 Survey for KSCRS Members: Current Trends in Cataract Surgery in Korea
- 2004 Survey for KSCRS Members: Current Trends in Cataract Surgery in Korea
- 2005 Survey for KSCRS Members: Current Trends in Cataract Surgery in Korea
- 2007 Survey for KSCRS Members: Current Trends in Cataract Surgery in Korea
