Removal of Eyelid Epidermal Cyst Using High-Frequency Radio-Wave Electrosurgery
- Affiliations
-
- 1Department of Ophthalmology, Dongguk University Gyeongju Hospital, Dongguk University College of Medicine, Gyeongju, Korea. ophho@hanmail.net
- KMID: 2338952
- DOI: http://doi.org/10.3341/jkos.2014.55.12.1727
Abstract
- PURPOSE
To introduce an effective new surgical approach with high-frequency radio-wave electrosurgery to remove eyelid epidermal cysts.
METHODS
Thirteen patients (13 eyes) with eyelid epidermal cysts were enrolled in the present study. All patients underwent high-frequency radio-wave electrosurgery (Ellman surgitron(R)) to remove the epidermal cyst. The results were analyzed retrospectively, after a follow-up of more than 6 months.
RESULTS
At 6 months postoperatively, all eyes showed no recurrence of epidermal cyst. Additionally, no complications were reported by any patient.
CONCLUSIONS
High-frequency radio-wave electrosurgery is an effective procedure to remove eyelid epidermal cyst without recurrence.
MeSH Terms
Figure
-
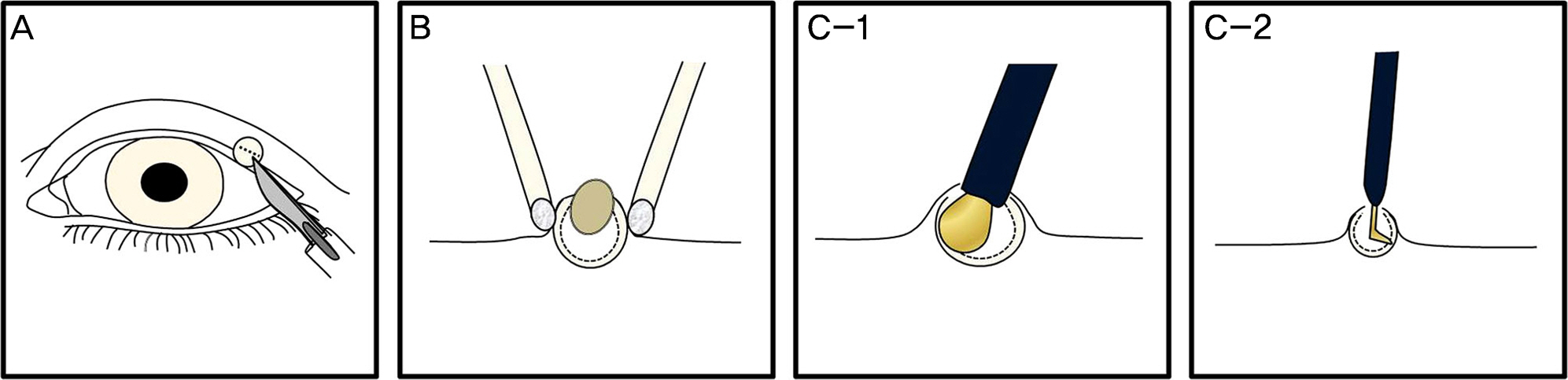
Figure 1. Schematic diagram of removing eyelid epidermal cysts with high-frequency radio-wave electrosurgery. With the tip of a No. 11 surgical blade, small linear incision is made on the top of epidermal cyst, penetrating the wall of the cyst (A). Uniform, centripetal pressure around the cyst using cotton-tipped applicator is applied at the base of the cyst to express the contents of the cyst, including part of the cyst wall (B). When the size of the cyst is larger than 2 mm, ball-type probe is inserted in the cyst, and the cyst is coagulated with high-frequency radio-wave electrosurgery for removal of potential residual epidermal sac (C-1). When the size is smaller than 2 mm, curved pin-type probe is inserted in the cyst and the capsule is coagulated for removal of potential residual sac (C-2).

Figure 2. Intraoperative photographs using ball-type electrode for epidermal cysts, larger than 2 mm. With the tip of a No. 11 surgical blade, small linear incision is made on the top of epidermal cyst (A). Centripetal pressure is applied at the base of the cyst, and the contents of the cyst is being exposed (B). The contents of the cyst are expressed (C). Ball-type electrode of adequate size is selected, and the cyst is coagulated with high-frequency radio-wave electrosurgery (D).
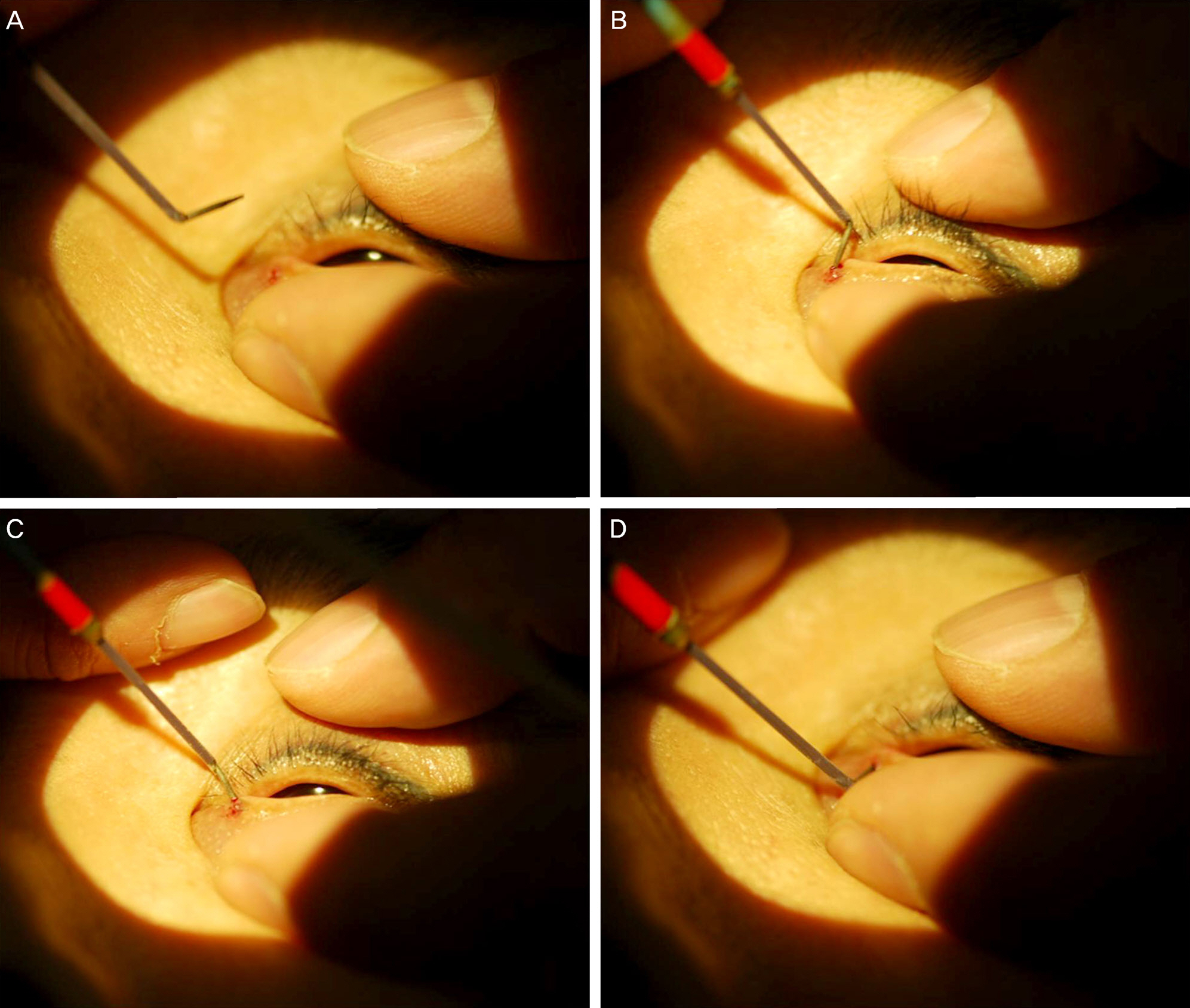
Figure 3. Intraoperative photographs using curved pin-type electrode for epidermal cysts, smaller than 2 mm. After the contents of the cyst are expressed, a pin-type electrode of adequate size is selected and the tip of electrode is curved (A). The tip of electrode is inserted and rotated in the cyst to coagulate the cyst wall (B, C, D).
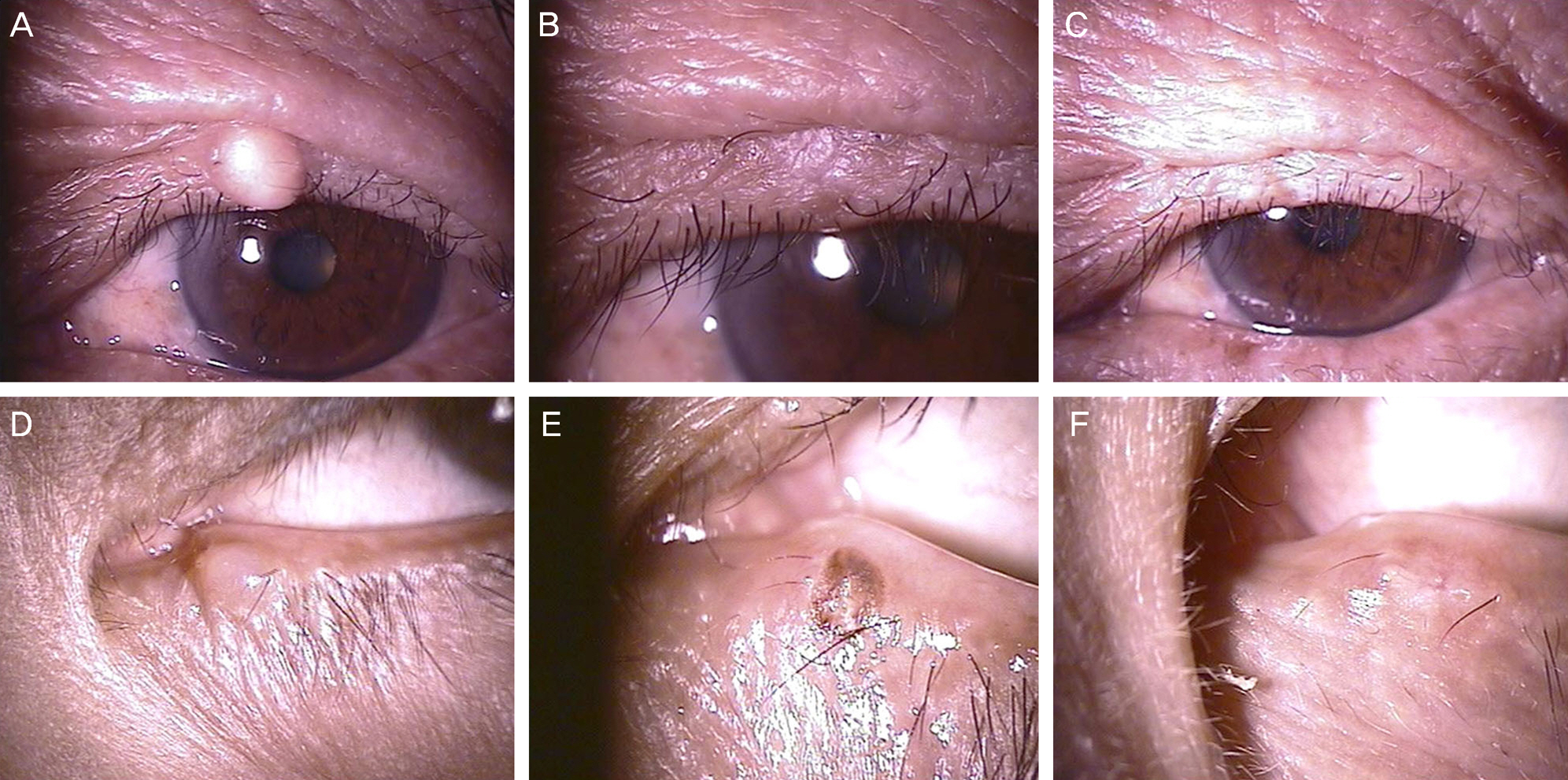
Figure 4. Slit-lamp photographs of the patients. Preoperative eyelid epidermal cyst (large epidermal cyst-A, small epidermal cyst-D), 1 week after removing epidermal cyst with high-frequency radio-wave electrosurgery (large epidermal cyst-B, small epidermal cyst-E), 1 month after removal of epidermal cyst with high-frequency radio-wave electrosurgery (large epidermal cyst-C, small epidermal cyst-F). Epidermal postinflammatory hyperpigmentation was observed at the electrosurgery site, 1 week after removing epidermal cyst (E). But it spontaneously faded at 1 month (F).
Cited by 1 articles
-
The Effects of Surgery for Conjunctival Lymphangiectasia Using a High-frequency Radio Wave Electrosurgical Unit
Hyun Kyo Jeong, Hyo Song Park, Kyoung Yul Seo, Jeihoon Lee
J Korean Ophthalmol Soc. 2018;59(4):314-318. doi: 10.3341/jkos.2018.59.4.314.
Reference
-
References
1. Kim SY, Park KY, Oh JW, et al. Epidermal and adnexal nevi and tumors. Korean Dermatology Association Textbook Editing Board. Dermatology. 6th ed.Seoul: Medbook;2014. chap. 26.2. Thomas VD, Snavely NR, Lee KK, et al. Benign epithelial tumors, hamartomas, and hyperplasias. Goldsmith LA, Katz SI, Gilchrest BA, editors. Fitzpatrick's dermatology in general medicine. 8th ed.Newyork: McGraw-Hill professional publishing;2012. chap. 118.3. Yanoff M, Sassani JW. Ocular pathology. 6th ed.Maryland Heights, Missouri: Mosby Elsevier;2009. p. 188–9.4. Itoh Y, Watanabe Y, Henta T, Ishibashi A. Endoscopic extraction and curettage of epidermal cysts on the face. Br J Plast Surg. 1999; 52:182–4.
Article5. Klin B, Ashkenazi H. Sebaceous cyst excision with minimal surgery. Am Fam Physician. 1990; 41:1746–8.6. Jordan DR. Multiple epidermal inclusion cysts of the eyelid: a simple technique for removal. Can J Ophthalmol. 2002; 37:39–40.
Article7. Moore C, Greer DM Jr. Sebaceous cyst extraction through mini-incisions. Br J Plast Surg. 1975; 28:307–9.
Article8. Yang HJ, Yang KC. A new method for facial epidermoid cyst removal with minimal incision. J Eur Acad Dermatol Venereol. 2009; 23:887–90.
Article9. Lucarelli MJ, Ahn HB, Kulkarni AD, Kahana A. Intratarsal epidermal inclusion cyst. Ophthal Plast Reconstr Surg. 2008; 24:357–9.
Article10. Vagefi MR, Lin CC, McCann JD, Anderson RL. Epidermoid cyst of the upper eyelid tarsal plate. Ophthal Plast Reconstr Surg. 2008; 24:323–4.
Article11. Kim TJ, Kim N, Park HJ, et al. A case of eyelid steatocystoma. J Korean Ophthalmol Soc. 2012; 53:1027–9.
Article12. Kronish JW, Sneed SR, Tse DT. Epidermal cysts of the eyelid. Arch Ophthalmol. 1988; 106:270.
Article13. Lieblich LM, Geronemus RG, Gibbs RC. Use of a biopsy punch for removal of epithelial cysts. J Dermatol Surg Oncol. 1982; 8:1059–62.
Article14. Lee HE, Yang CH, Chen CH, et al. Comparison of the surgical outcomes of punch incision and elliptical excision in treating epidermal inclusion cysts: a prospective, randomized study. Dermatol Surg. 2006; 32:520–5.
Article15. Mehrabi D, Leonhardt JM, Brodell RT. Removal of keratinous and pilar cysts with the punch incision technique: analysis of surgical outcomes. Dermatol Surg. 2002; 28:673–7.
Article16. Notowicz A. Treatment of lesions of steatocystoma multiplex and other epidermal cysts by cryosurgery. J Dermatol Surg Oncol. 1980; 6:98–9.17. Vivakananthan C. Minimal incision for removing sebaceous cysts. Br J Plast Surg. 1972; 25:60–2.
Article18. Zuber TJ. Minimal excision technique for epidermoid (sebaceous) cysts. Am Fam Physician. 2002; 65:1409–12. 1417–8. –1420.19. Oliveira AS, Picoto AS, Verde SF, Martins O. A simple method of excising tricholemmal cysts from the scalp. J Dermatol Surg Oncol. 1979; 5:625–7.
Article20. Hurwitz JJ, Johnson D, Howarth D, Molgat YM. Experimental treatment of eyelashes with high-frequency radio wave electrosurgery. Can J Ophthalmol. 1993; 28:62–4.21. Suh JS, Choi S. The effect of conjunctivochalasis surgery using a high-frequency radio-wave electrosurgical unit. J Korean Ophthalmol Soc. 2012; 53:1571–6.
Article22. Youm DJ, Kim JM, Choi CY. Simple surgical approach with high-frequency radio-wave electrosurgery for conjunctivochalasis. Ophthalmology. 2010; 117:2129–33.
Article23. Huang SK. Advances in applications of radiofrequency current to catheter ablation therapy. Pacing Clin Electrophysiol. 1991; 14:28–42.
Article24. Han KE, Choi CY, Seo KY. Removal of lymphangiectasis using high-frequency radio wave electrosurgery. Cornea. 2013; 32:547–9.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two Cases of Corneal Neovascularization Treatment Using High-frequency Radio Wave Electrosurgery
- Evaluation of Subconjunctival Remnant Particles after High-frequency Radio-wave Electrosurgery for Conjunctivochalasis
- Treatment of Trichiasis and Districhiasis with Ellman Dento-Surg 90FFP
- Acute Exacerbation of Conjunctival Papilloma after High-frequency Radio Wave Electrosurgery for Conjunctivochalasis: A Case Report
- The Effect of Conjunctivochalasis Surgery Using a High-Frequency Radio-Wave Electrosurgical Unit
