J Korean Ophthalmol Soc.
2013 Oct;54(10):1508-1513.
Comparison of Clinical Outcomes Between Torsional Phacoemulsification of Infiniti(R) and Longitudinal Phacoemulification of Stellaris(R) Through 2.2 mm Microincision
- Affiliations
-
- 1Department of Ophthalmology & Visual Science College of Medicine, The Catholic University of Korea, Seoul, Korea. sara514@catholic.ac.kr
Abstract
- PURPOSE
To compare clinical outcomes of a 2.2 mm microcoaxial cataract surgery, using torsional mode and longitudinal mode.
METHODS
In this comparative study, patients with bilateral cataract were assigned to get microcoaxial cataract surgery by torsional mode of infiniti in one eye and longitudinal mode of Stellaris(R) in the other eye. Primary outcome measures were US time (UST), cumulative dissipated energy (CDE), mean amount of balanced salt solution (BSS) used and surgical complications. Patients were seen 1, 7, 30, and 60 days after surgery. Postoperative outcome measures were the final best corrected visual acuity (BCVA), central corneal thickness (CCT), endothelial cell count and surgically induced astigmatism (SIA).
RESULTS
The study evaluated 68 eyes of 34 patients (nuclear opalescence (NO)2: 40 eyes, and NO3: 28 eyes). CDE was significantly lower in torsional mode (3.52 +/- 2.93) than in longitudinal mode (6.20 +/- 3.32) (p = 0.001). Torsional mode (60.88 +/- 21.18 ml) had more BSS use than longitudinal mode (34.58 +/- 13.54 ml) (p < 0.001). There were no significant differences in postoperative BCVA, CCT change, endothelial change, and SIA (p > 0.05).
CONCLUSIONS
The torsional mode may provide lower level of phacoemulsification energy than the longitudinal mode and Torsional mode is considered effective and safe phacoemulsification. However the surgical outcomes were not significantly different in 2.2 mm microcoaxial cataract surgery of moderate cataract. So surgeon can choose any phaco machine based on experience and preference.
Keyword
MeSH Terms
Figure
-
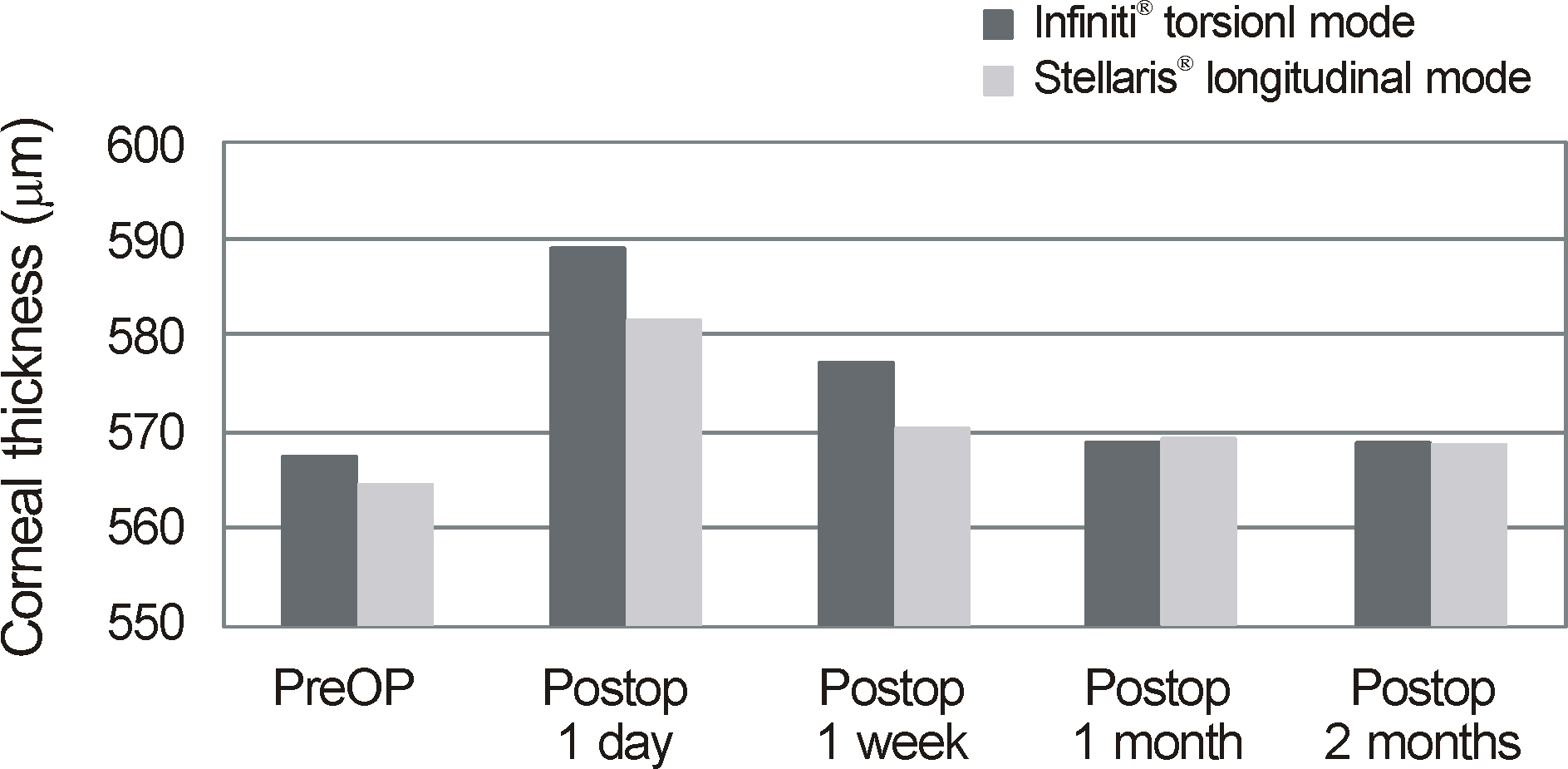
Figure 1. Change of preoperative and postpoerative central corneal thickness µm).

Figure 2. Change in corneal endothelial cell density (cells/mm2).
Reference
-
References
1. Hoffman RS, Fine IH, Packer M. New phacoemulsification technology. Curr Opin Ophthalmol. 2005; 16:38–43.
Article2. Storr-Paulsen A, Norregaard JC, Ahmed S. . Endothelial cell damage after cataract surgery: divide-and-conquer versus pha- co-chop technique. J Cataract Refract Surg. 2008; 34:996–1000.3. Davison JA, Cionni RJ, Snowdon JR. . Simultaneous surgeon and side-view video analysis comparing in situ fracture and stop- and-chop phacoemulsification. J Cataract Refract Surg. 2005; 31:274–9.4. Walkow T, Anders N, Klebe S. Endothelial cell loss after phacoemulsification: relation to preoperative and intraoperative parameters. J Cataract Refract Surg. 2000; 26:727–32.
Article5. Fishkind W, Bakewell B, Donnenfeld ED. . Comparative clinical trial of ultrasound phacoemulsification with and without the WhiteStar system. J Cataract Refract Surg. 2006; 32:45–9.
Article6. Wong T, Hingorani M, Lee V. Phacoemulsification time and power requirements in phaco chop and divide and conquer nucleofractis techniques. J Cataract Refract Surg. 2000; 26:1374–8.
Article7. Kim DH, Wee WR, Lee JH, Kim MK. The comparison between torsional and conventional mode phacoemulsification in moderate and hard cataracts. Korean J Ophthalmol. 2010; 24:336–40.
Article8. Liu Y, Zeng M, Liu X. . Torsional mode versus conventional ultrasound mode phacoemulsification: randomized comparative clinical study. J Cataract Refract Surg. 2007; 33:287–92.9. Holladay JT, Cravy TV, Koch DD. Calculating the surgically induced refractive change following ocular surgery. J Cataract Refract Surg. 1992; 18:429–43.
Article10. Hayashi K, Hayashi H, Nakao F, Hayashi F. Risk factors for corneal endothelial injury during phacoemulsification. J Cataract Refract Surg. 1996; 22:1079–84.
Article11. Reuschel A, Bogatsch H, Barth T, Wiedemann R. Comparison of endothelial changes and power settings between torsional and longitudinal phacoemulsification. J Cataract Refract Surg. 2010; 36:1855–61.
Article12. Werblin TP. Long-term endothelial cell loss following phacoemulsification: model for evaluating endothelial damage after intraocular surgery. Refract Corneal Surg. 1993; 9:29–35.
Article13. Kreisler KR, Mortenson SW, Mamalis N. Endothelial cell loss following “modern” phacoemulsification by a senior resident. Ophthalmic Surg. 1992; 23:158–60.
Article14. Bissen-Miyajima H. Ophthalmic viscosurgical devices. Curr Opin Ophthalmol. 2008; 19:50–4.
Article15. Berdahl JP, Jun B, DeStafeno JJ, Kim T. Comparison of a torsional handpiece through microincision versus standard clear corneal cataract wounds. J Cataract Refract Surg. 2008; 34:2091–5.
Article16. Polack FM, Sugar A. The phacoemulsification procedure. II. Corneal endothelial changes. Invest Ophthalmol. 1976; 15:458–69.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of Clinical Outcomes between Torsional and Longitudinal Phacoemulsification
- Comparison of Influences on the Cornea by the Longitudinal Phacoemulsification Between the Sovereign(R) and Infiniti(R)
- The Comparison between Torsional and Conventional Mode Phacoemulsification in Moderate and Hard Cataracts
- Surgical Outcomes of Intravitreal Torsional Phacoemulsification for Dropped Lens Fragments during Cataract Surgery
- Comparison of Surgically-induced Astigmatism after Combined Phacoemulsification and 23-Gauge Vitrectomy: 2.2-mm vs. 2.75-mm Cataract Surgery
