A Case of Suprasellar Arachnoid Cyst with Compressive Optic Neuropathy
- Affiliations
-
- 1Department of Ophthalmology, Pusan National University College of Medicine, Busan, Korea. alertlee@hanmail.net
- 2Department of Radiology, Pusan National University College of Medicine, Busan, Korea.
Abstract
- PURPOSE
To report a case of suprasellar arachnoid cyst with compressive optic neuropathy.
CASE SUMMARY
A 50-year-old man presented with decreased visual acuity in the right eye of 6 months duration. Best corrected visual acuity was 0.2 in the right eye, 1.0 in the left eye, and the intraocular pressure was 13 mm Hg in the right eye, and 18 mm Hg in the left eye. Fundus examination showed pale optic disc in the right eye and retinal nerve fiber layer defects in both eyes. Visual field examination revealed a central visual field of 10degrees in the right eye and an inferior visual field defect in the left eye. The brain magnetic resonance image (MRI) showed a suprasellar arachnoid cyst that compressing the optic nerve and chiasm.
CONCLUSIONS
The author experienced arachnoid cyst accompanied by optic disc atrophy and visual field defect in a patient diagnosed and treated for glaucoma. In cases of non-specific clinical features that differ from typical glaucomatous presentations, the utilization of brain MRI appears to be helpful in diagnosis and treatment.
MeSH Terms
Figure
-

Figure 1 Retinal nerve fiber layer (RNFL) and disc photographs of the patient at initial visit. Cup-disc ratio is 0.68 in the right eye (A) and 0.52 in the left eye (B). Greater pallor than cupping is observed in the optic disc of the right eye (A). Diffuse RNFL defects in the right eye (C). Note superior and inferior RNFL defects, but a relatively intact neuroretinal rim in left eye (D).
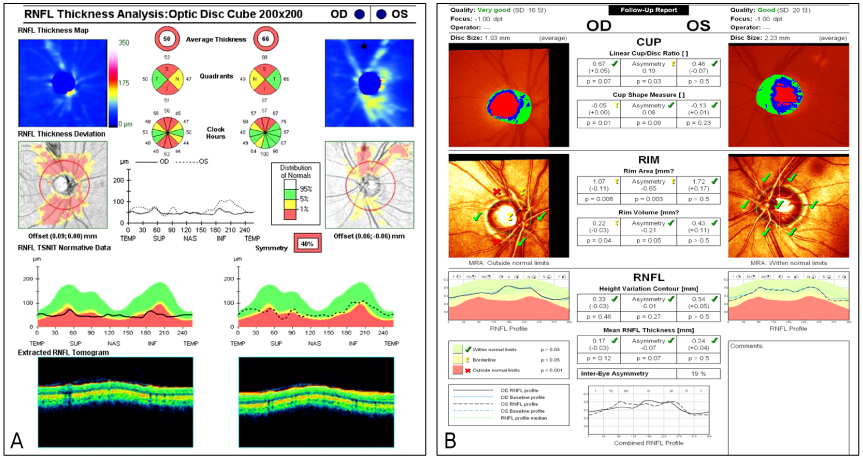
Figure 2 Optical coherence tomography (OCT) (A) and Heidelberg retinal tomography (HRT) (B). Diffuse retinal nerve fiber layer defects were detected in the RNFL thickness deviation map on OCT in the right eye with abnormal Moorfield Regression Analysis (MRA) on HRT. There are superior and inferior RNFL defects on the RNFL thickness deviation map of OCT in the left eye with normal MRA on HRT.

Figure 3 Note the infero-nasal step defect in the left eye (A) and inferior altitudinal and superior arcuate visual field defects in the right eye (B) at initial visit. After 18 months, the visual field index (VFI) and mean deviation (MD) decreased in both eyes and pattern standard deviation (PSD) increased in the both eyes (C, D). Central visual field remained within 10° at initial visit, but it decreased within 5° after 18 months.

Figure 4 P100 amplitude of right eye decreased more severely than that of the left eye and P100 latency delayed in both eyes.

Figure 5 The patient's brain MRI. (A) Transverse T2-weighted scan shows suprasellar cistern enlargement due to arachnoid cysts (black arrowheads). (B) Coronal T2-weighted scan shows elevated optic nerve (red arrow), elongated pituitary stalk (black arrow) due to arachnoid cyst (black arrowheads). (C) Sagittal T1-weighted scan shows optic nerve compression (red arrow) due to arachnoid cyst (white arrowheads).
Reference
-
1. Cheng CH, Lin HL, Cho DY, et al. Intracavernous sinus arachnoid cyst with optic neuropathy. J Clin Neurosci. 2010. 17:267–269.2. Choi JU, Kim DS, Huh R. Endoscopic approach to arachnoid cyst. Childs Nerv Syst. 1999. 15:285–291.3. Thompson TP, Lunsford LD, Kondziolka D. Successful management of sellar and suprasellar arachnoid cysts with stereotatic intracavitary irradiation: an expanded report of four cases. Neurosurgery. 2000. 46:1518–1522.4. Kim CS, Seong GJ, Lee NH, et al. Prevalence of primary open-angle glaucoma in central South Korea the Namil study. Ophthalmology. 2011. 118:1024–1030.5. Iwase A, Suzuki Y, Araie M, et al. The prevalence of primary open-angle glaucoma in Japanese: the Tajimi Study. Ophthalmology. 2004. 111:1641–1648.6. Stamper RL, Lieberman MF, Drake MV, editors. Primary open angle glaucoma. Becker-Shaffer's Diagnosis and Therapy of the Glaucoma. 2009. 8th ed. St. Louis: Mosby Elsevier;chap. 17.7. Allingham RR, Damji KF, Freedman S, Moro SE, Rhee DJ, editors. Chronic open-angle glaucoma and normal-tension glaucoma. Shields Textbook of Glaucoma. 2011. 6th ed. Philadelphia: Lippincott Williams & Wilkins;chap. 11.8. Sadun AA, Win PH, Ross-Cisneros FN, et al. Leber's hereditary optic neuropathy differentially affects smaller axons in the optic nerve. Trans Am Ophthalmol Soc. 2000. 98:223–232.9. Danesh-Meyer HV, Papchenko T, Savino PJ, et al. In vivo retinal nerve fiber layer thickness measured by optical coherence tomography predicts visual recovery after surgery for parachiasmal tumors. Invest Ophthalmol Vis Sci. 2008. 49:1879–1885.10. Heijl A, Bengtsson B, Hyman L, et al. Natural history of open-angle glaucoma. Ophthalmology. 2009. 116:2271–2276.11. Byeon SH, Hong WP, Ahn JH, Park BW. A case of visual field defect from intracranial optic nerve compressio by normal caliber internal carotid artery. J Korean Ophthalmol Soc. 2004. 45:1956–1960.12. Jung JW, Jin HC, Kim KS, Kim YC. A case of compressive optic neuropathy due to breast cancer metastasis. J Korean Ophthalmol Soc. 2010. 51:1161–1165.13. Kim I, Kim M, Chung Y. A case of compressive optic neuropathy caused by sphenoid sinus mucocele. J Korean Ophthalmol Soc. 1989. 30:1025–1029.14. Rubin RM, Alfredo AS, Alfio P. Yanooff M, Ducker JS, editors. Optic chiasm, parasellar region, and pituitary fossa. Yanooff and Ducker Ophthalmology. 2009. 3rd ed. China: Elsevier;chap. 9.11.15. Kaisho Y, Miyazaki S, Shimo-oku M, et al. [A case of suprasellar arachnoid cyst followed up for a long time]. Nihon Ganka Gakkai Zasshi. 1995. 99:109–114.16. Chang JK, Kyung SE, Jang MH, et al. A case of arachnoid cyst with floating symptom. J Korean Ophthalmol Soc. 2009. 50:481–485.17. Greenfield DS, Siatkowski RM, Glaser JS, et al. The cupped Disc. Who needs neuroimaging? Ophthalmology. 1998. 105:1866–1874.18. Fujiwara M, Bitoh S, Hasegawa H, Ohtsuki H. [A case of intrasellar arachnoid cyst]. No Shinkei Geka. 1984. 12:331–337.19. Yadav YR, Parihar V, Sinha M, Jain N. Endoscopic treatment of the suprasellar arachnoid cyst. Neurol India. 2010. 58:280–283.20. Beier AD, Cheshier SH, Chakraborty A, Dirks P. Suprasellar arachnoid cyst resulting in the syndrome of inappropriate antidiuretic hormone secretion. J Neurosurg Pediatr. 2010. 6:486–488.21. Cincu R, Agrawal A, Eiras J. Intracranial arachnoid cysts: Current concepts and treatment alternatives. Clin Neurol Neurosurg. 2007. 109:837–843.
