A Case of Orbital Abscess with Central Retinal Artery Occlusion
- Affiliations
-
- 1Department of Ophthalmology, Konyang University College of Medicine, Daejeon, Korea. hmseye@hanmail.net
Abstract
- PURPOSE
To report a case of rapidly progressed orbital abscess after central retinal artery occlusion.
CASE SUMMARY
A 60-year-old man with right periorbital pain and edema starting 3 days earlier visited the hospital. His first visual acuity was 1.0 for the right eye with peripheral edema and tenderness; severe hemorrhagic chemosis, proptosis (approximately 3 mm) and extraocular motility limitation were also observed. According to the CT findings, a 2.5 x 1 cm-sized encapsulated cystic mass was found in the right orbital cavity, along the medial orbital wall; with a diagnosis of orbital abscess, he was hospitalized with systemic antibiotic treatment and abscess drainage. On the second day of hospitalization, the best corrected visual acuity was reduced to light perception, and relative afferent pupillary defect, pale retina and cherry red spot were found. Therefore, emergent incisional drainage, optic massage, and antibiotics were given to the patient. Immediately after the surgery, the peripheral edema and proptosis improved; nevertheless, central retinal artery occlusion did not resolve and vision did not improve. Two months later, best corrected visual acuity for the right eye was counting fingers and central retinal artery occlusion showed no further improvement.
CONCLUSIONS
No case report on rapidly progressing orbital abscess has been proposed in Korea to date. In the case of rapidly progressed orbital abscess, incisional drainage and antibiotics should be administered promptly.
MeSH Terms
Figure
-

Figure 1 External photograph demonstrates severe lid swelling, erythema and hemorrhagic chemosis at admission.

Figure 2 CT scans demonstrate inferolateral displacement of the right eyeball by an orbital abscess (35 × 10 mm) that extends along the medial orbital wall (HD #1). Mild right ethmoiditis and no evidence of carvenous sinus thrombosis.

Figure 3 Fundus photograph shows some retinal hemorrhage and retinal edema with cherry-red spot in the right eye (HD #2).

Figure 4 Fundus photograph and OCT show consistent retinal hemorrhage with cherry-red spot and retinal edema (POD #11).
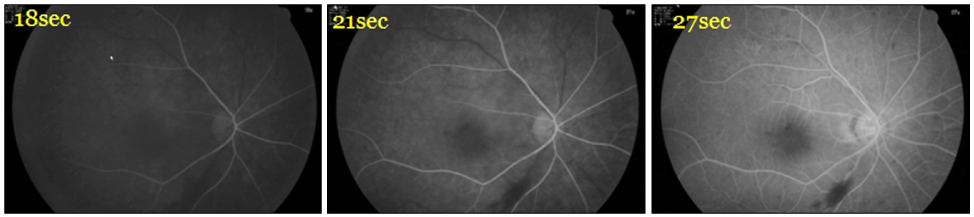
Figure 5 Fluorescein angiographs show delayed arterial filling in the right eye (POD #11).

Figure 6 The patient 11 days after the operation. Decreased lid swelling and proptosis, but remained exodeviation of right eye (A). The patient 2 months 11 days after the operation. No lid swelling or proptosis (B).
Reference
-
1. Chandler JR, Langenbrunner DJ, Stevens ER. The pathogenesis of orbital complications in acute sinusitis. Laryngoscope. 1970. 80:1414–1428.2. Dolman PJ, Glazer LC, Harris GJ, et al. Mechanisms of visual loss in severe proptosis. Ophthal Plast Reconstr Surg. 1991. 7:256–260.3. Alvi NP, Mafee M, Edward DP. Ophthalmic artery occlusion following orbital inflammation: a clinical and histopathological study. Can J Ophthalmol. 1998. 33:174–179.4. Pond F, Berkowitz RG. Superolateral subperiosteal orbital abscess complicating sinusitis in a child. Int J Pediatr Otorhinolaryngol. 1999. 48:255–258.5. Ataullah S, Sloan B. Acute dacryocystitis presenting as an orbital abscess. Clin Experiment Ophthalmol. 2002. 30:44–46.6. Youssef OH, Stefanyszyn MA, Bilyk JR. Odontogenic orbital cellulitis. Ophthal Plast Reconstr Surg. 2008. 24:29–35.7. Rootman J. Diseases of the Orbit. A Multidisciplinary Approach. 2003. 2nd ed. Philadelphia: Lippincott Williams & Wilkins;467.8. Sobol SE, Marchand J, Tewfik TL, et al. Orbital complications of sinusitis in children. J Otolaryngol. 2002. 31:131–136.9. Harris GJ. Subperiosteal abscess of the orbit: older children and adults require aggressive treatment. Ophthal Plast Reconstr Surg. 2001. 17:395–397.10. Krohel GB, Krauss HR, Winnick J. Orbital abscess. Presentation, diagnosis, therapy, and sequelae. Ophthalmology. 1982. 89:492–498.11. Younis RT, Anand VK, Davidson B. The role of computed tomography and magnetic resonance imaging in patients with sinusitis with complications. Laryngoscope. 2002. 112:224–229.12. Tanenbaum M, Tenzell J, Byrne SF, Forster RK. Medical management of orbital abscess. Surv Ophthalmol. 1985. 30:211–212.13. Ferguson MP, McNab AA. Current treatment and outcome in orbital cellulitis. Aust N Z J Ophthalmol. 1999. 27:375–379.14. Reddy SC, Sharma HS, Mazidah AS, et al. Orbital abscess due to acute ethmoiditis in a neonate. Int J Pediatr Otorhinolaryngol. 1999. 49:81–86.15. Coşkun M, Ilhan Ö, Keskin U, et al. Central retinal artery occlusion secondary to orbital cellulitis and abscess following dacryocystitis. Eur J Ophthalmol. 2011. 21:649–652.16. Okamoto Y, Hiraoka T, Okamoto F, Oshika T. A case of subperiosteal abscess of the orbit with central retinal artery occlusion. Eur J Ophthalmol. 2009. 19:288–291.17. Cho HS, Kwon JW, Ahn HS. Central retinal artery occlusion and orbital abscess following dental abscess. J Korean Ophthalmol Soc. 2003. 44:750–754.18. Koo NK, Kim JH, Lee SY. A case of bilateral cavernous sinus thrombosis with intraorbital abscess. J Korean Ophthalmol Soc. 2005. 46:731–735.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Central Retinal Artery Occlusion and Orbital Abscess following Dental Abscess
- Incomplete Central Retinal Artery Occlusion
- The Successful Treatment of a Case of Central Retinal Artery Occlusion
- Central Retinal Artery Occlusion after Cervical Spine Surgery in Prone Position: A Case Report
- A Case of Cilioretinal Artery Occlusion Associated with Central Retinal Vein Occlusion
