Ocular Ischemic Syndrome Successfully Treated With Carotid Angioplasty and Stenting
- Affiliations
-
- 1Department of Ophthalmology, Gyeongsang National University School of Medicine, Jinju, Korea. parkjm@gnu.ac.kr
- 2Gyeongsang Institute of Health Science, Gyeongsang National University, Jinju, Korea.
Abstract
- PURPOSE
To report a case of ocular ischemic syndrome successfully treated with delayed carotid angioplasty and stenting (CAS).
CASE SUMMARY
A 52-year-old male was admitted to our hospital because of amaurosis fugax-like symptoms in the right eye for several months. His visual acuity was 0.8 in the right eye and he did not have rubeosis iridis. Neovascularization of the disc, narrowing of the retinal artery and multiple retinal hemorrhages were diagnosed by fundus examination. Fluorescein angiography showed delayed choroidal filling, a delayed arm-to-retina time, prolongation of arteriovenous transit time, neovascularization of the disc, retinal capillary nonperfusion, and staining of the retinal vessels. MR angiography showed severe stenosis in the proximal portion of the right carotid artery. We diagnosed this case as ocular ischemic syndrome. The patient was recommended carotid angioplasty and stenting at the severely narrowed portion of the right carotid artery, but it was postponed about six months after diagnosis because of personal problems. At the final follow-up, 24 months after stenting, the amaurosis fugax symptoms had disappeared, the patient had an improved visual acuity of 1.0, and the new vessels on the disc changed to fibrous tissue. Fluorescein angiography showed resolution of the delayed arm-to-retina time and prolongation of the arteriovenous transit time, disappearances of the leakage around the disc and the retinal capillary nonperfusion.
MeSH Terms
Figure
-
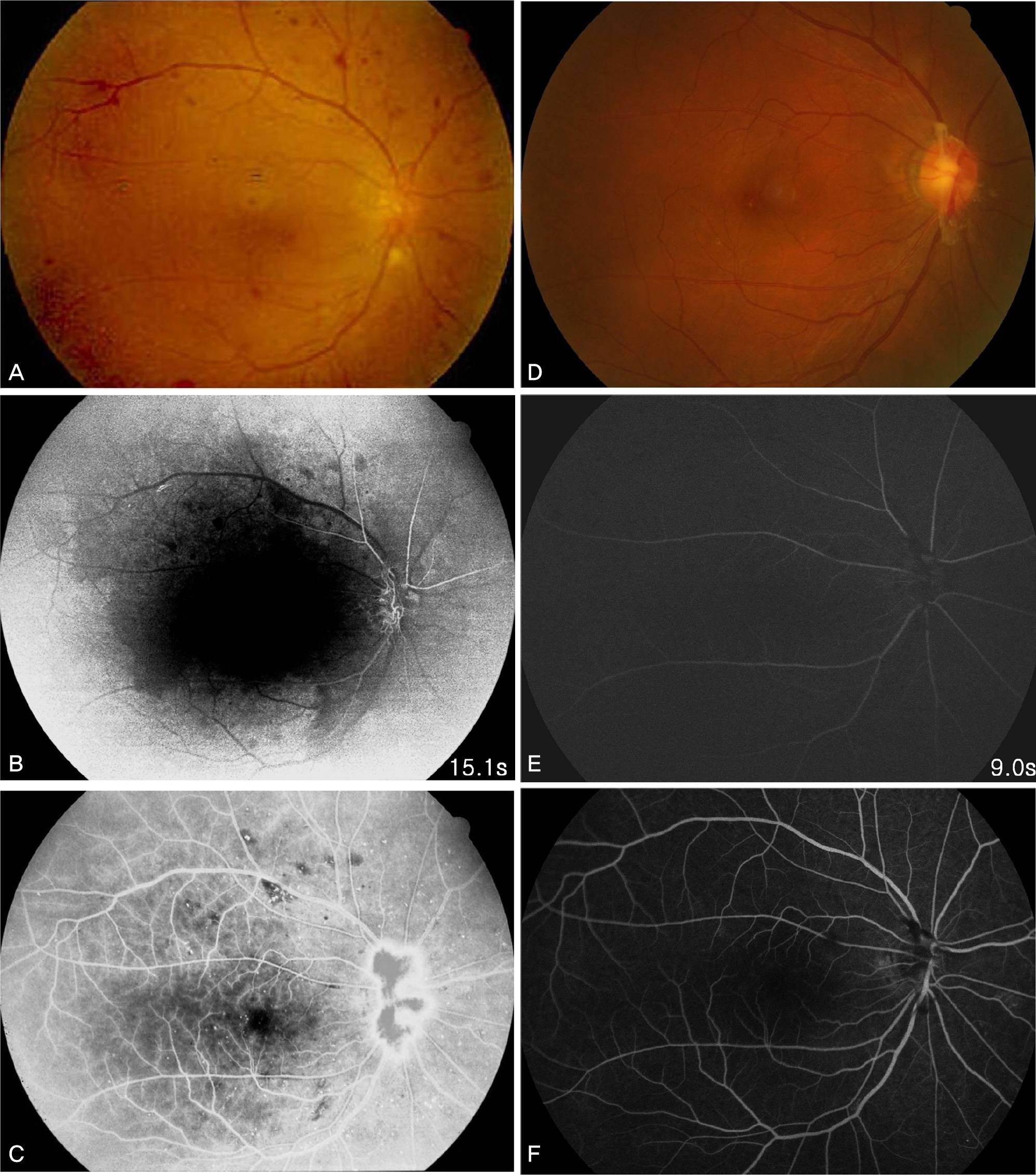
Figure 1. Fundus photograph and fluorescein angiography in the early and late phase before (A, B, C) and after (D, E, F) carotid angioplasty and stenting (CAS). (A) Before CAS, fundus photograph shows multiple dot retinal hemorrhage and arterial narrowing. (B) Early phase in fluorescein angiography shows delayed arm-to-retina time and new vessels on disc. (C) Late phase shows leakage from new vessels on the disc and reveals non-perfusion area. (D) After CAS, fundus photograph shows disappearance of new vessels in the disc which is changed to fibrous tissue. (E) Early phase in fluorescein angiography shows disappearance of new vessels on the disc and no delayed arm-to-retina time. (F) Late phase shows no leakage from the disc and well perfused entire retina.
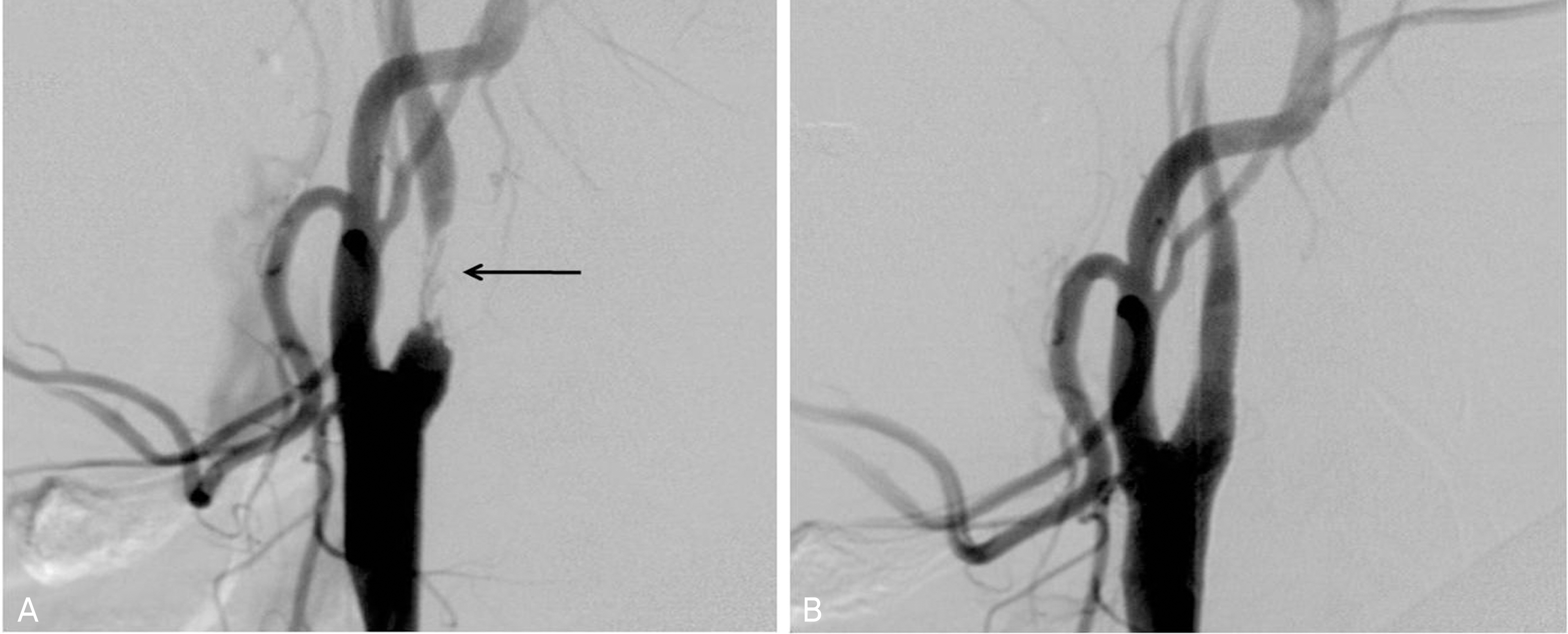
Figure 2. Carotid angiography before (A) and after (B) carotid angioplasty and stenting (CAS). (A) Before CAS, the right internal carotid artery shows stenosis more than 90% but, (B) after CAS, successful stenting and good flow are shown (arrow: stenotic site of the carotid artery).

Figure 3. CT angiography and reconstructed three dimensional image before (A, B) and after (C, D) carotid angioplasty and stenting (CAS). Before CAS, the lumen of the right carotid artery is stenotic with artheroma (A) and not visible in reconstructed image (B) but after CAS, the lumen is well enhanced with contrast material (C) and well visible in the reconstructed image (D).
Reference
-
References
1. Kearns TP, Hollenhorst RW. Venous-stasis retinopathy of occlusive disease of the carotid artery. Proc Staff Meet Mayo Clin. 1963; 38:304–12.2. Brown GC, Magargal LE. The ocular ischemic syndrome. Clinical, fluorescein angiographic and carotid angiographic features. Int Ophthalmol. 1988; 11:239–51.3. Mun SJ, Lee KH, Lee DU, Cho NC. Clinical features of ophthalmic artery hypoperfusion. J Korean Ophthalmol Soc. 2007; 48:297–302.4. Sivalingam A, Brown GC, Megargal LE. The ocular ischemic syndrome II. Visual prognosis and the effect of treatment. Int Ophthalmol. 1991; 15:15–20.5. Amselem L, Montero J, Diaz-Llopis M, et al. Intravitreal bevacizumab injection in ocular ischemic syndrome. Am J Ophthalmol. 2007; 144:122–4.6. Wholey MH. Wholey M. Current status in cervical carotid artery stent placement. J Cardiovasc Surg. 2003; 44:331–9.7. Marx JL, Hreib K, Choi IS, et al. Percutaneous carotid artery angioplasty and stenting for ocular ischemic syndrome. Ophthalmology. 2004; 111:2284–91.
Article8. Costa VP, Kuzniec S, Molnar LJ, et al. Clinical findings and hemodynamic changes associated with severe occlusive carotid artery disease. Ophthalmology. 1997; 104:1994–2002.
Article9. Sarkies NJ, Shilling JS, Russell RW. Fluorescein angiography in carotid disease. Trans Ophthalmol Soc U K. 1986; 105:489–93.10. Bosley TM. The role of carotid noninvasive tests in stroke. Semin Neurol. 1986; 6:194–203.11. Palmowski AM, Ruprecht KW. Amaurosis fugax. Fortschr Med. 1992; 110:531–5.12. Suwanwela NC, Chutinetr A. Risk factors for atherosclerosis of cervicocerebral arteries: intracranial versus extracranial. Neuro-epidemiology. 2003; 22:37–40.
Article13. Kawaguchi S, Sakaki T, Iwahashi H, et al. Effect of carotid artery stenting on ocular circulation and chronic ocular ischemic syndrome. Cerebrovasc Dis. 2006; 22:402–8.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Treatment of Acute Central Retinal Artery Occlusion with Ocular Ischemic Syndrome
- A Case of Transseptal Approach to Carotid Artery Stenting in Right Internal Carotid Stenosis
- Delayed Carotid Wallstent Shortening Resulting in Restenosis Following Successful Carotid Artery Angioplasty and Stenting
- Current Indications of Surgery and Endovascular Treatment in Ischemic Stroke
- A Case of Ocular Ischemic Syndrome Associated with Multiple Branch Retinal Artery Occlusion and Neovascular Glaucoma
