The Supraorbital Approach to a Large Retrobulbar Cavernous Hemangioma of the Orbit-One Case Report
- Affiliations
-
- 1Department of Ophthalmology, Hanyang University College of Medicine, Seoul, Korea. lyjot@hanyang.ac.kr
- 2Department of Neurosurgery, Hanyang University College of Medicine, Seoul, Korea.
Abstract
- PURPOSE
To report a complete excision of a large superior orbital retrobulbar cavernous hemangioma using supraorbital craniotomy through the suprabrow approach combined with superior orbital wall removal.
CASE SUMMARY
A 31-year-old woman presented to our clinic with left exophthalmos beginning one month earlier. Visual acuities and intraocular pressures of both eyes were normal and there was no diplopia and no limitation in ocular movement. On exophthalmometry, the right eye was 15 mm and the left eye was 18 mm. CT and MRI demonstrated a superior orbital retrobulbar mass of 2.0x2.6x2.0 cm in size, and the mass displaced the superior rectus and levator palpebrae muscles. After six months, a neurosurgeon attempted a classic supraorbital craniotomy but failed. Fourteen months later, the authors completely excised the tumor through superior orbital wall removal. The tumor was confirmed as a cavernous hemangioma after histopathologic study.
CONCLUSIONS
The authors succeeded in complete excision of a superior orbital retrobulbar cavernous hemangioma using supraorbital craniotomy through a suprabrow approach combined with superior orbital wall removal.
MeSH Terms
Figure
-

Figure 1. Fourteen months after classic supraorbital craniotomy failed, CT scan with enhancement was obtained. (A) Sagittal view. The mass is well marginated, sized by 2.0×2.6×2.4 cm. (B) Coronal view. The mass deviates the optic nerve downward and abuts on the superior rectus muscle. Contrasted study shows that the mass is enhanced at the delayed phase.
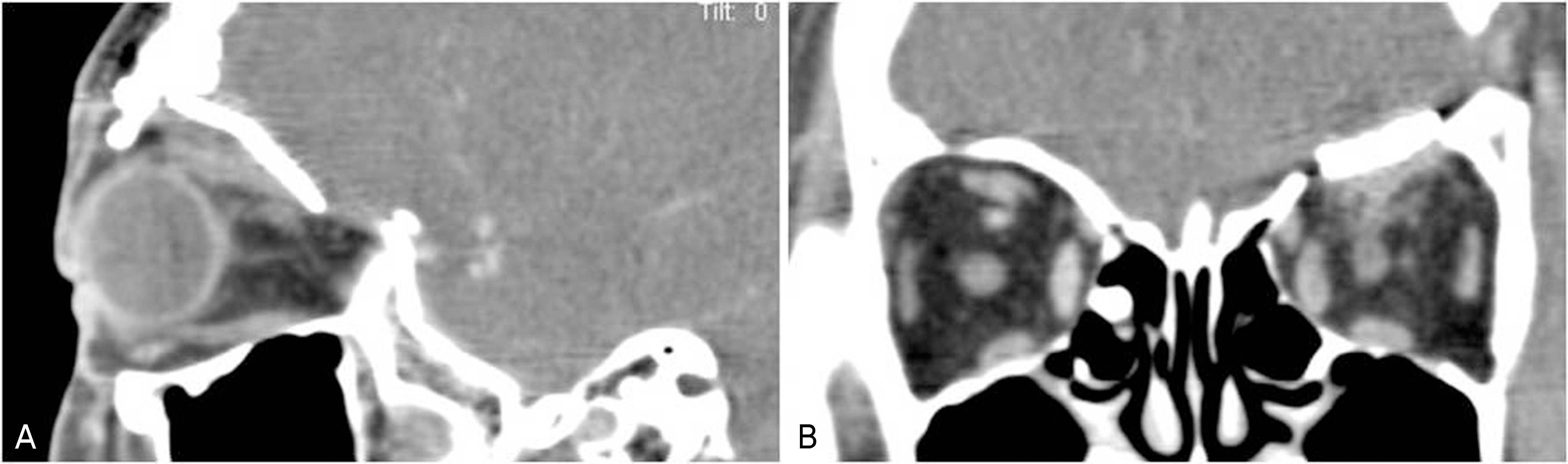
Figure 2. A and B. Six months after the tumor was removed, CT scan with enhancement was obtained. There is no evidence of tumor remnant or tumor recurrence.
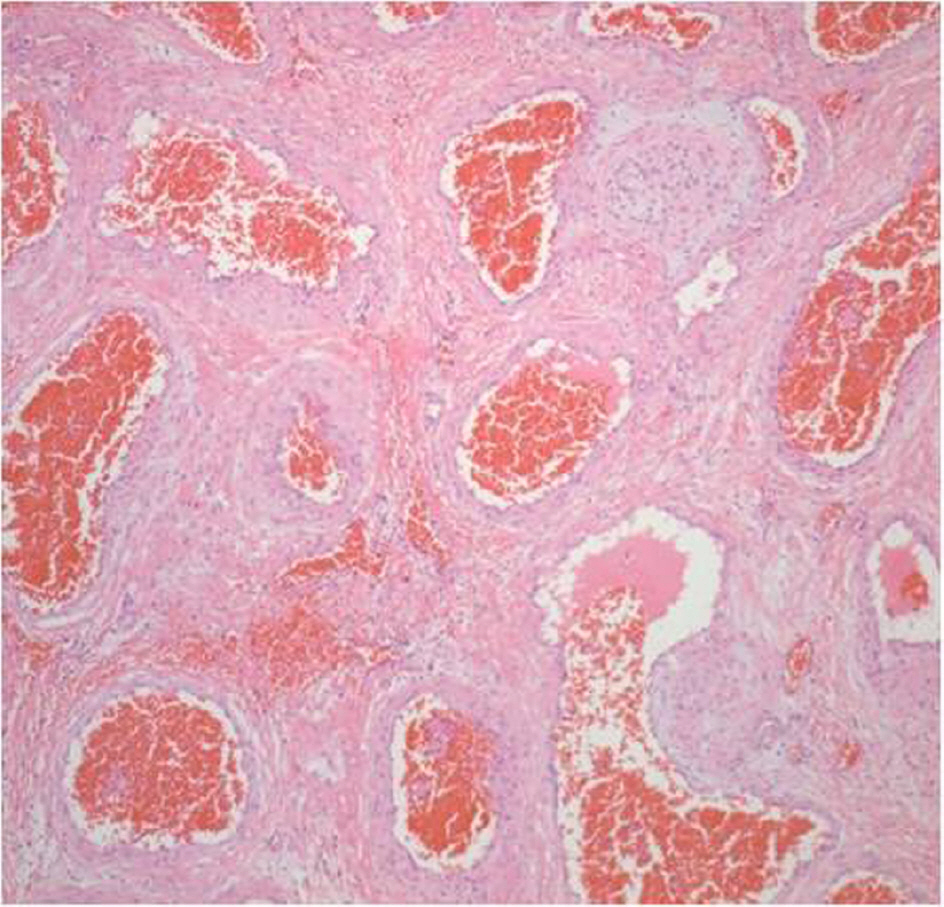
Figure 3. Histopathological findings representing a cavernous hemangioma of the orbit. Hematoxylin and eosin stain (×100).
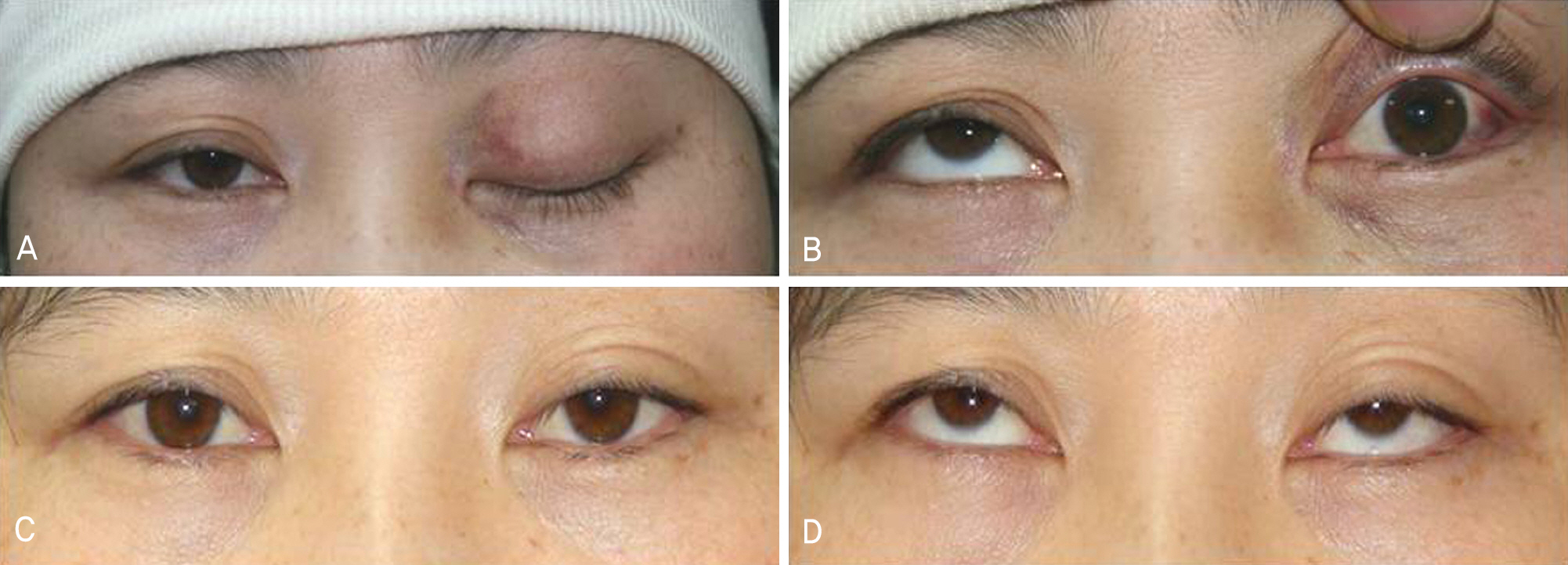
Figure 4. A and B. On the first postoperative day, the patient shows complete ptosis and severe upper gaze limitation in the left eye. C and D. After 6 months, the patient shows mild ptosis and normal upper gaze movement.

Figure 5. Diagram of a supraorbital craniotomy combined with superior orbital wall removal is outlined using dotted blue line on a three-dimensional CT reconstruction image. (Black line means incision line of classic supraorbital craniotomy, black ellipse means burr hole in the temporal fossa and red circle means the tumor).
Reference
-
References
1. Reese AB. Tumors of the eye. 3rd ed.Hagerstown: Harper & Row;1976. p. 272.2. Rootman J. Diseases of the orbit. A multidisciplinary approach. 2nd ed.Philadelphia: Lippincott Williams & Wilkins;2003. p. 420–60.3. Scheuerle AF, Steiner HH, Kolling G, et al. Treatment and longterm outcome of patients with orbital cavernomas. Am J Ophthalmol. 2004; 138:237–44.
Article4. Rootman J. Vascular malformations of the orbit: hemodynamic concepts. Orbit. 2003; 22:103–20.
Article5. Harris GJ, Perez N. Surgical sectors of the orbit: using the lower fornix approach for large, medial intraconal tumors. Ophthal Plast Reconstr Surg. 2002; 18:349–54.
Article6. Park JH, Jin SJ, Lim CS. A case of orbital cavernous hemangioma with multiple intracranial lesions. J Korean Ophthalmol Soc. 2000; 41:2497–501.7. Limawararut V, Davis G, Crompton J, et al. Recurrent multiple cavernous hemangiomas of the orbit in association with systemic tumors. Am J Ophthalmol. 2006; 141:943–5.
Article8. McNab AA, Wright JE. Cavernous haemangiomas of the orbit. Aust N Z J Ophthalmol. 1989; 17:337–45.
Article9. Jacobiec FA, Jones IS. Clinical Ophthalmology: Vascular tumor, malformation and degenerations. Philadelphia: Harper & Row;1983. p. 1–14.10. Rootman J. Vascular lesions, diseases of the orbit. 1st ed.Philadelphia: JB Lippincott;1988. p. 522–3.11. Choi YJ, Lee JI, Kim YD. Gamma knife radiosurgery for orbital lesions. J Korean Ophthalmol Soc. 2008; 49:555–61.
Article12. Yanoff M, Fine BS. Orbit, ocular pathology. 3rd ed.Philiadelphia: JB Lippincott;1989. p. 522–3.13. Kronlein RU. Pathology and surgery of the orbital cysts. Beitr Klein Chir. 1889; 4:149–63.14. Brusati R, Goisis M, Biglioli F, et al. Surgical approaches to cavernous haemangiomas of the orbit. Br J Oral Maxillofac Surg. 2007; 45:457–62.
Article15. Nesi FA, Lisman RD, Levine MR. Ophthalmic plastic and reconstructive surgery. 2nd ed.St. Louis: Mosby;1998. p. 861–9.16. Nerad JA. Oculoplastic surgery. St. Louis: Mosby;2001. p. 387–418.17. Cutney C, Bernardino CR, Buono LM, et al. Transorbital craniotomy through a suprabrow approach: A case series. Orbit. 2001; 20:107–17.
Article18. Joseph V, Chacko AG. Suprabrow minicraniotomy for suprasellar tumours. Br J Neurosurg. 2005; 19:33–7.
Article19. Goldberg RA, Shorr N, Arnold AC, Garcia GH. Deep transorbital approach to the apex and cavernous sinus. Ophthal Plast Reconstr Surg. 1998; 14:336–41.
Article20. Lew HL, Lee SY, Lee KS, et al. Removal of orbital tumor through transfrontal approach. J Korean Ophthalmol Soc. 1994; 35:1723–7.21. Schmidek HH, Roberts DW. Operative neurosurgical techniques. 5th ed.Philadelphia: Saunders;2006. p. 159–60.
